Ganesan Sarada, Xavier Joseph
Department of Surgery, Wollongong Hospital, Wollongong, New South Wales, Australia.
Department of Surgery, Wollongong Hospital, Wollongong, New South Wales, Australia.
Int J Surg Case Rep. 2023 Sep;110:108705. doi: 10.1016/j.ijscr.2023.108705. Epub 2023 Aug 20.
Colorectal intussusception can be quite challenging to identify, especially its malignant nature. This is a fairly rare presentation and hence, there is not much associated research or cases reported in the literature.
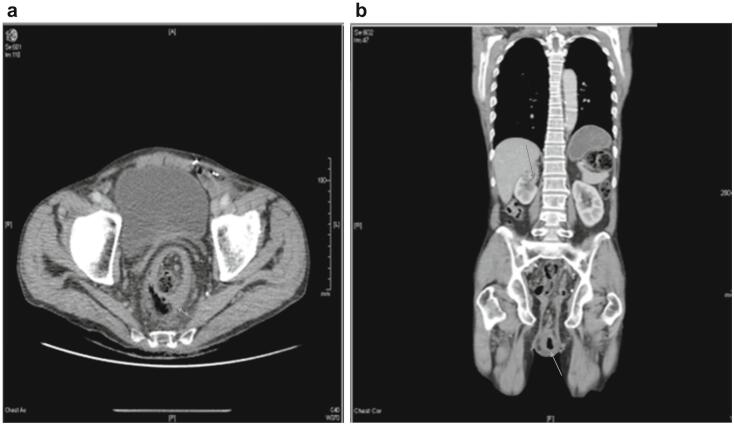
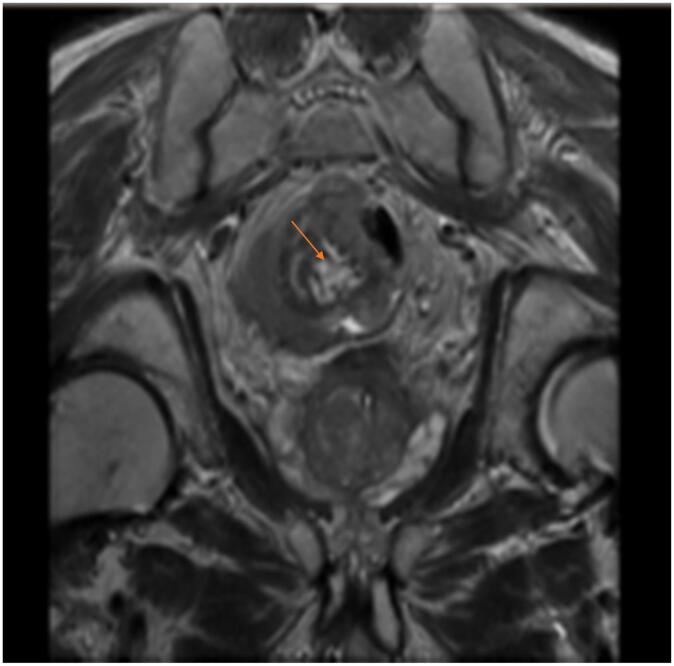
We present a 69 year old male with lower abdominal pain and a significant rectal prolapse. He has a background history of heavy smoking and significant alcohol intake. The prolapse was irreducible and had papillomatous changes present on the prolapsed mucosa. A computerized tomography (CT) scan demonstrated a large rectal prolapse followed by a Magnetic Resonance Imaging (MRI) Pelvis which showed an intussusception at the S2-3 level, consistent with a carcinoma, The patient then proceeded to have a flexible sigmoidoscopy with a planned proceed to an anterior resection. Histopathology revealed sigmoid and descending colon adenocarcinoma with mucinous differentiation pT3N0. He had an unremarkable hospital stay and remained well on follow up. His case was discussed at the multidisciplinary meeting and was not for any adjuvant chemotherapy.
Imaging can help aid early diagnosis of a colorectal intussusception. Colonoscopies can be useful too; however these can be tricky to diagnose pre-operatively. If there is a high suspicion of malignancy, routine resection is the preferred method of treatment in cases of colorectal intussusception.
Although not a very common presentation, diagnosis of colorectal cancer presenting as an intussusception can be dealt with imminently by considering operative measures.
结直肠套叠的识别颇具挑战性,尤其是其恶性性质。这是一种相当罕见的表现,因此,文献中相关研究或病例报道不多。
我们报告一例69岁男性,有下腹部疼痛及明显的直肠脱垂。他有大量吸烟和大量饮酒的病史。脱垂无法回纳,脱垂黏膜有乳头状改变。计算机断层扫描(CT)显示巨大直肠脱垂,随后盆腔磁共振成像(MRI)显示S2 - 3水平套叠,符合癌表现。患者随后接受了乙状结肠镜检查,并计划进行前切除术。组织病理学显示乙状结肠和降结肠腺癌伴黏液分化,pT3N0。他住院过程顺利,随访情况良好。他的病例在多学科会议上进行了讨论,无需进行辅助化疗。
影像学有助于结直肠套叠的早期诊断。结肠镜检查也可能有用;然而,术前诊断可能较棘手。如果高度怀疑恶性,对于结直肠套叠病例,常规切除是首选治疗方法。
尽管结直肠癌表现为套叠并非常见情况,但通过考虑手术措施,可立即处理此类诊断。