Department of Health Sciences (DISSAL), University of Genoa, Genoa, Italy.
Infectious Diseases Unit, San Martino Policlinico Hospital - IRCCS for Oncology and Neurosciences, L.go R. Benzi 10, 16132, Genoa, Italy.
Crit Care. 2023 Aug 24;27(1):323. doi: 10.1186/s13054-023-04608-1.
Pneumocystis jirovecii pneumonia (PJP) is an opportunistic, life-threatening disease commonly affecting immunocompromised patients. The distribution of predisposing diseases or conditions in critically ill patients admitted to intensive care unit (ICU) and subjected to diagnostic work-up for PJP has seldom been explored.
The primary objective of the study was to describe the characteristics of ICU patients subjected to diagnostic workup for PJP. The secondary objectives were: (i) to assess demographic and clinical variables associated with PJP; (ii) to assess the performance of Pneumocystis PCR on respiratory specimens and serum BDG for the diagnosis of PJP; (iii) to describe 30-day and 90-day mortality in the study population.
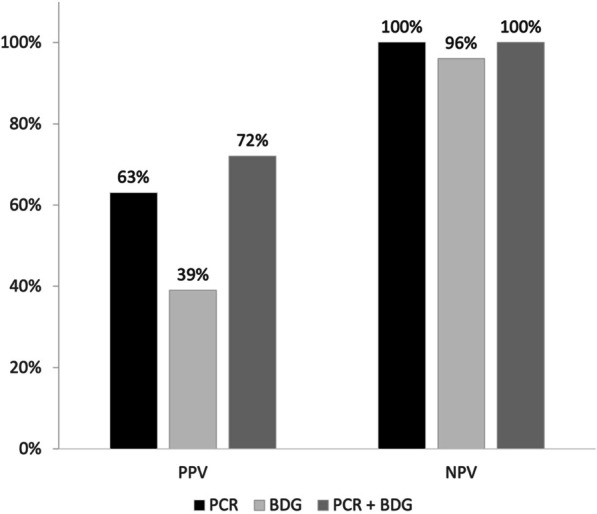
Overall, 600 patients were included in the study, of whom 115 had presumptive/proven PJP (19.2%). Only 8.8% of ICU patients subjected to diagnostic workup for PJP had HIV infection, whereas hematological malignancy, solid tumor, inflammatory diseases, and solid organ transplants were present in 23.2%, 16.2%, 15.5%, and 10.0% of tested patients, respectively. In multivariable analysis, AIDS (odds ratio [OR] 3.31; 95% confidence interval [CI] 1.13-9.64, p = 0.029), non-Hodgkin lymphoma (OR 3.71; 95% CI 1.23-11.18, p = 0.020), vasculitis (OR 5.95; 95% CI 1.07-33.22, p = 0.042), metastatic solid tumor (OR 4.31; 95% CI 1.76-10.53, p = 0.001), and bilateral ground glass on CT scan (OR 2.19; 95% CI 1.01-4.78, p = 0.048) were associated with PJP, whereas an inverse association was observed for increasing lymphocyte cell count (OR 0.64; 95% CI 0.42-1.00, p = 0.049). For the diagnosis of PJP, higher positive predictive value (PPV) was observed when both respiratory Pneumocystis PCR and serum BDG were positive compared to individual assay positivity (72% for the combination vs. 63% for PCR and 39% for BDG). Cumulative 30-day mortality and 90-day mortality in patients with presumptive/proven PJP were 52% and 67%, respectively.
PJP in critically ill patients admitted to ICU is nowadays most encountered in non-HIV patients. Serum BDG when used in combination with respiratory Pneumocystis PCR could help improve the certainty of PJP diagnosis.
卡氏肺孢子虫肺炎(PJP)是一种机会性的、危及生命的疾病,常见于免疫功能低下的患者。在重症监护病房(ICU)接受诊断性检查的危重症患者中,易患疾病或情况的分布情况很少被探讨。
本研究的主要目的是描述接受卡氏肺孢子虫诊断性检查的 ICU 患者的特征。次要目标是:(i)评估与 PJP 相关的人口统计学和临床变量;(ii)评估呼吸道标本和血清 BDG 中卡氏肺孢子虫 PCR 对 PJP 的诊断性能;(iii)描述研究人群的 30 天和 90 天死亡率。
总体而言,共有 600 名患者纳入研究,其中 115 例患者有疑似/确诊的 PJP(19.2%)。仅 8.8%的接受 PJP 诊断性检查的 ICU 患者存在 HIV 感染,而血液系统恶性肿瘤、实体瘤、炎症性疾病和实体器官移植在接受检查的患者中分别占 23.2%、16.2%、15.5%和 10.0%。多变量分析显示,艾滋病(比值比 [OR] 3.31;95%置信区间 [CI] 1.13-9.64,p=0.029)、非霍奇金淋巴瘤(OR 3.71;95% CI 1.23-11.18,p=0.020)、血管炎(OR 5.95;95% CI 1.07-33.22,p=0.042)、转移性实体瘤(OR 4.31;95% CI 1.76-10.53,p=0.001)和 CT 扫描双侧磨玻璃影(OR 2.19;95% CI 1.01-4.78,p=0.048)与 PJP 相关,而淋巴细胞计数增加呈负相关(OR 0.64;95% CI 0.42-1.00,p=0.049)。对于 PJP 的诊断,与单个检测阳性相比,呼吸道卡氏肺孢子虫 PCR 和血清 BDG 均阳性时观察到更高的阳性预测值(PPV)(联合检测为 72%,PCR 为 63%,BDG 为 39%)。疑似/确诊 PJP 患者的 30 天累积死亡率和 90 天死亡率分别为 52%和 67%。
目前,在入住 ICU 的危重症患者中,卡氏肺孢子虫肺炎最常发生在非 HIV 患者中。当与呼吸道卡氏肺孢子虫 PCR 联合使用时,血清 BDG 有助于提高 PJP 诊断的确定性。