Department of Cardiothoracic Surgery, Lancashire Cardiac Centre, Blackpool Victoria Hospital, Blackpool, UK.
School of Science, Engineering and Environment, University of Salford, Manchester, UK.
J Cardiothorac Surg. 2023 Aug 24;18(1):252. doi: 10.1186/s13019-023-02303-4.
Performing wedge resection rather than lobectomy for primary lung cancer remains controversial. Recent studies demonstrate no survival advantage for non-anatomical resection compared to lobectomy in patients with early-stage lung cancer. The objective of this study was to investigate whether in patients with T1 tumours, non-anatomical wedge resection is associated with equivalent survival to lobectomy.
This was a retrospective cohort study of patients who underwent lung resection at the Lancashire Cardiac Centre between April 2005 and April 2018. Patients were subjected to multidisciplinary team discussion. The extent of resection was decided by the team based on British Thoracic Society guidelines. The primary outcome was overall survival. Propensity matching of patients with T1 tumours was also performed to determine whether differences in survival rates exist in a subset of these patients with balanced pre-operative characteristics.
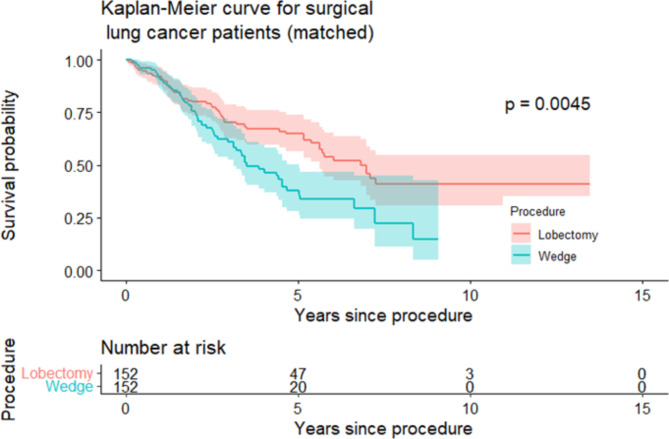
There were 187 patients who underwent non-anatomical wedge resection and 431 patients who underwent lobectomy. Cox modelling demonstrated no survival difference between groups for the first 1.6 years then a risk of death 3-fold higher for wedge resection group after 1.6 years (HR 3.14, CI 1.98-4.79). Propensity matching yielded 152 pairs for which 5-year survival was 66.2% for the lobectomy group and 38.5% for the non-anatomical wedge group (SMD = 0.58, p = 0.003).
Non-anatomical wedge resection was associated with significantly reduced 5-year survival compared to lobectomy in matched patients. Lobectomy should remain the standard of care for patients with early-stage lung cancer who are fit enough to undergo surgical resection.
对于原发性肺癌,行楔形切除术而非肺叶切除术仍然存在争议。最近的研究表明,与肺叶切除术相比,非解剖性切除术在早期肺癌患者中并未带来生存优势。本研究的目的是探讨对于 T1 肿瘤患者,非解剖性楔形切除术是否与肺叶切除术具有相当的生存获益。
这是一项回顾性队列研究,纳入了 2005 年 4 月至 2018 年 4 月期间在兰开夏心脏中心接受肺切除术的患者。患者均经多学科团队讨论。切除范围由团队根据英国胸科学会指南决定。主要结局为总生存。对 T1 肿瘤患者进行倾向评分匹配,以确定在这些患者的亚组中,是否存在生存差异。
有 187 例患者行非解剖性楔形切除术,431 例患者行肺叶切除术。Cox 模型分析显示,两组在前 1.6 年内无生存差异,然后在 1.6 年后楔形切除术组的死亡风险高 3 倍(HR 3.14,CI 1.98-4.79)。倾向评分匹配得到 152 对,其中肺叶切除术组 5 年生存率为 66.2%,非解剖性楔形切除术组为 38.5%(SMD=0.58,p=0.003)。
在匹配患者中,与肺叶切除术相比,非解剖性楔形切除术与显著降低的 5 年生存率相关。对于适合接受手术切除的早期肺癌患者,肺叶切除术仍应作为标准治疗方法。