Neuroradiology Unit, NESMOS Department Sant'Andrea Hospital, La Sapienza University of Rome, Via di Grottarossa, 1035-1039, 00189 Rome, Italy.
Neuroradiology Unit, Imaging Department, Bambino Gesù Children's Hospital, Piazza Sant'Onofrio 4, 00165 Rome, Italy.
Tomography. 2023 Aug 18;9(4):1526-1537. doi: 10.3390/tomography9040122.
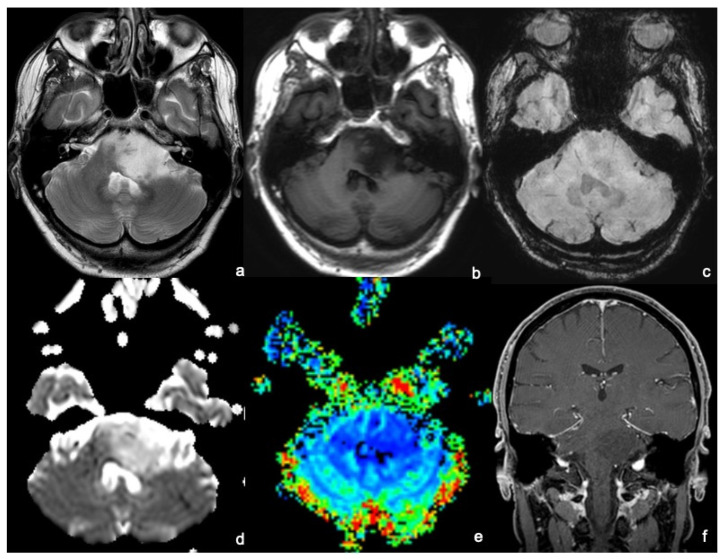
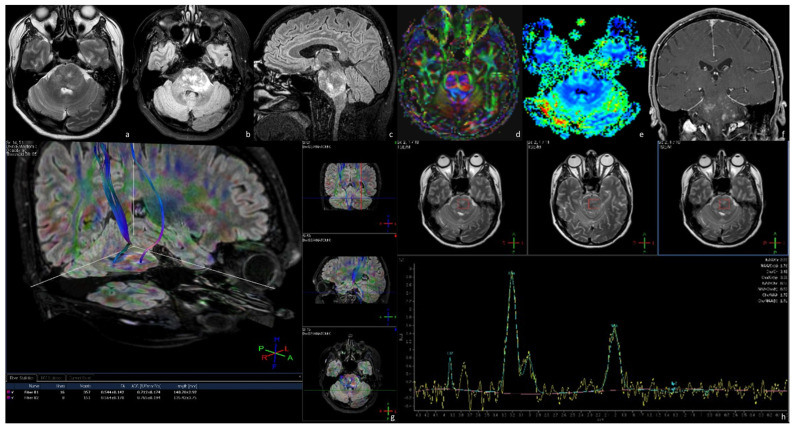
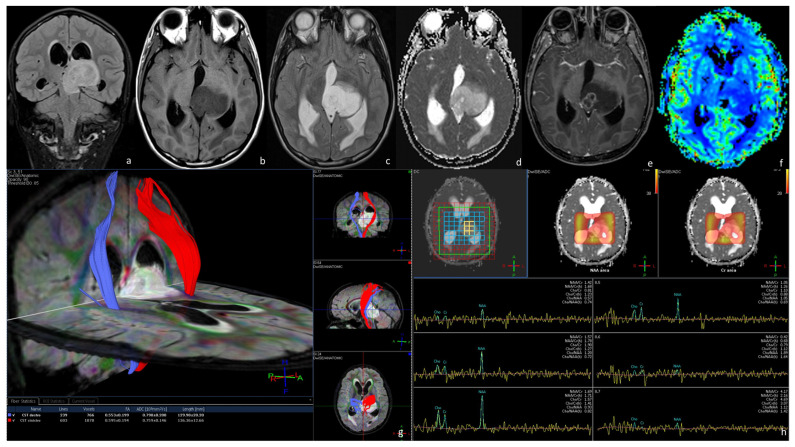
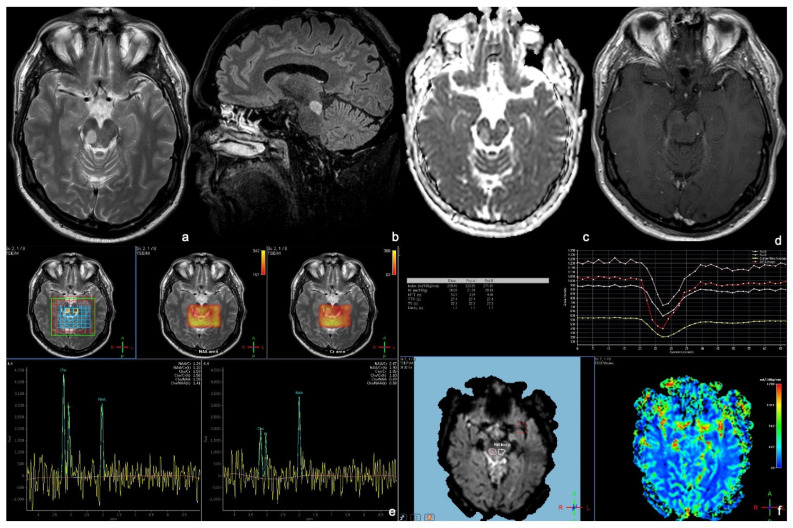
The 2021 WHO (World Health Organization) classification of brain tumors incorporated the rapid advances in the molecular, genetic, and pathogenesis understanding of brain tumor pathogenesis, behavior, and treatment response. It revolutionized brain tumor classification by placing great emphasis on molecular types and completely splitting adult-type and pediatric-type diffuse gliomas. Brainstem gliomas (BSGs) are the leading primary tumors of the brainstem, although they are quite uncommon in adults compared with the pediatric population, representing less than 2% of adult gliomas. Surgery is not always the treatment of choice since resection is rarely feasible and does not improve overall survival, and biopsies are not generally performed since the location is treacherous. Therefore, MRI (Magnetic Resonance Imaging) without and with gadolinium administration represents the optimal noninvasive radiological technique to suggest brainstem gliomas diagnosis, plan a multidisciplinary treatment and for follow-up evaluations. The MRI protocol encompasses morphological sequences as well as functional and advanced sequences, such as DWI/ADC (Diffusion-Weighted Imaging/Apparent Diffusion Coefficient), DTI (Diffusion Tensor Imaging), PWI (Perfusion-Weighted Imaging), and MRS (Magnetic Resonance Spectroscopy), which improve the accuracy of the diagnosis of BSGs by adding substantial information regarding the cellularity, the infiltrative behavior toward the v fiber tracts, the vascularity, and the molecular changes. Brainstem gliomas have been divided into four categories on the basis of their MRI radiological appearance, including diffuse intrinsic low-grade gliomas, enhancing malignant gliomas, localized tectal gliomas, and other forms. The aim of our review is to provide insight into the role of advanced MRI sequences in the diagnosis and follow-up of adult brainstem gliomas.
2021 年世界卫生组织(WHO)脑肿瘤分类纳入了脑肿瘤发病机制、行为和治疗反应的分子、遗传和发病机制方面的快速进展。它通过高度重视分子类型并完全拆分成人型和儿童型弥漫性神经胶质瘤,彻底改变了脑肿瘤分类。脑干胶质瘤(BSG)是脑干的主要原发性肿瘤,尽管与儿科人群相比,成人 BSG 相当罕见,仅占成人胶质瘤的不到 2%。由于切除很少可行且不能改善总体生存率,手术并不总是首选治疗方法,并且由于位置险恶,通常不进行活检。因此,不包括钆增强的 MRI(磁共振成像)是建议脑干胶质瘤诊断、制定多学科治疗计划和随访评估的最佳无创影像学技术。MRI 方案包括形态学序列以及功能和高级序列,例如 DWI/ADC(扩散加权成像/表观扩散系数)、DTI(扩散张量成像)、PWI(灌注加权成像)和 MRS(磁共振波谱),这些序列通过增加有关细胞密度、向 v 纤维束浸润行为、血管生成和分子变化的实质性信息,提高了 BSG 诊断的准确性。BSG 基于其 MRI 影像学表现分为四类,包括弥漫性固有低级别胶质瘤、强化恶性胶质瘤、局限性顶盖胶质瘤和其他形式。我们综述的目的是深入了解高级 MRI 序列在成人脑干胶质瘤的诊断和随访中的作用。