Department of Urology, Urology Research Institute, The First Affiliated Hospital of Fujian Medical University, Fuzhou, China.
Department of Urology, National Region Medical center, Binhai Campus of the First Affiliated Hospital, Fujian Medical University, Fuzhou, China.
Int Braz J Urol. 2023 Nov-Dec;49(6):716-731. doi: 10.1590/S1677-5538.IBJU.2023.0312.
Accurate preoperative prediction of adverse pathology is crucial for treatment planning of renal cell carcinoma (RCC). Previous studies have emphasized the potential of prostate-specific membrane antigen positron emission tomography / computed tomography (PSMA PET/CT) in differentiating between benign and malignant localized renal tumors. However, there is a scarcity of case reports elucidating the identification of aggressive pathological features using PET/CT. Our study was designed to prospectively compare the diagnostic value of enhanced CT, 68Ga-PSMA-11 and 18F-fluorodeoxyglucose (18F-FDG) PET/CT in clear-cell renal cell carcinoma (ccRCC) with necrosis or sarcomatoid or rhabdoid differentiation.
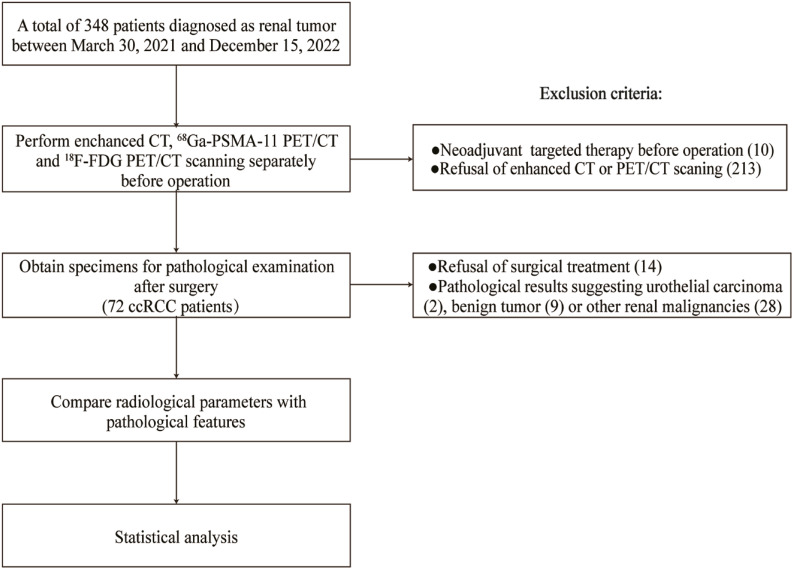
A prospective case series of patients with a newly diagnosed renal mass who underwent enhanced CT, 68Ga-PSMA-11 and 18F-FDG PET/CT within 30 days prior to nephrectomy was included. Complete preoperative and postoperative clinicopathological data were recorded. Patients who received neoadjuvant targeted therapy, declined enhanced CT or PET/CT scanning, refused surgical treatment or had non-ccRCC pathological indications were excluded. Radiological parameters were compared within subgroups of pathological characteristics. Bonferroni corrections were used to adjust for multiple testing and statistical significance was set at a p-value less than 0.017.
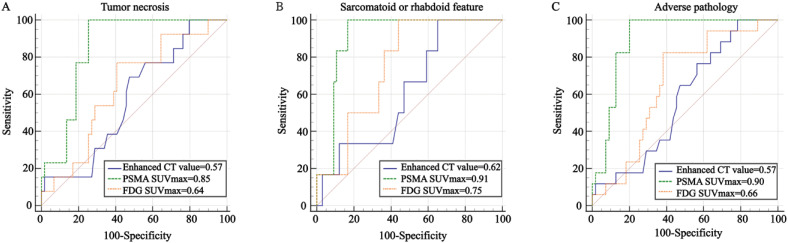
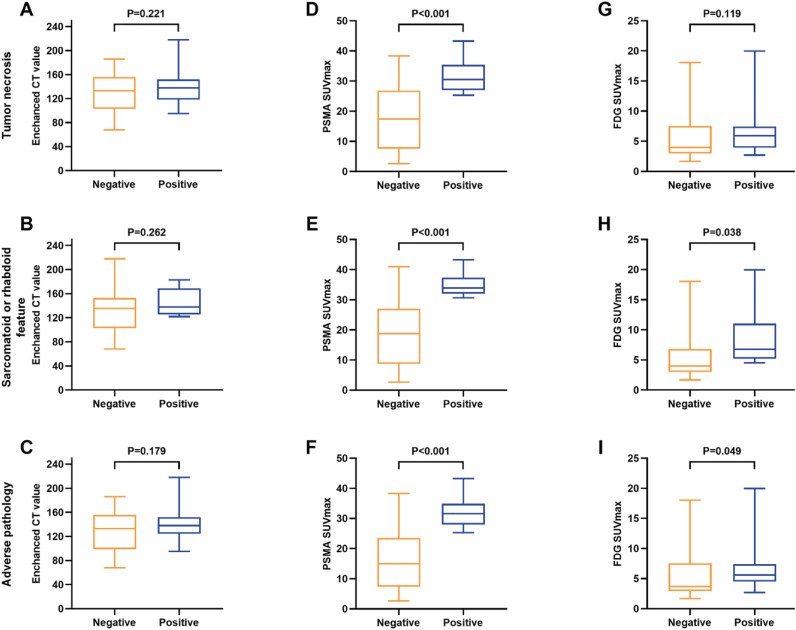
Seventy-two patients were available for the final analysis. Enhanced CT demonstrated poor performance in identifying necrosis, sarcomatoid or rhabdoid differentiation and adverse pathology (all P > 0.05). The maximum standardized uptake value (SUVmax) of 68Ga-PSMA-11 PET/CT was more effective than 18F-FDG PET/CT in identifying tumor necrosis and adverse pathology, with an area under the curve (AUC) of 0.85 (cutoff value=25.26, p<0.001; Delong test z=2.709, p=0.007) for tumor necrosis and AUC of 0.90 (cutoff value=25.26, p<0.001; Delong test z=3.433, p<0.001) for adverse pathology. However, no significant statistical difference was found between 68Ga-PSMA-11 and 18F-FDG PET/CT in predicting sarcomatoid or rhabdoid feature (AUC of 0.91 vs.0.75, Delong test z=1.998, p=0.046). Subgroup analyses based on age, sex, tumor location, maximal diameter, stage and WHO/ISUP grade demonstrated that 68Ga-PSMA-11 PET/CT SUVmax had a significant predictive value for adverse pathology. Enhanced CT value and SUVmax demonstrated strong reliability [intraclass correlation coefficient (ICC) > 0.80], indicating a robust correlation.
68Ga-PSMA-11 PET/CT demonstrates distinct advantages in identifying aggressive pathological features of primary ccRCC when compared to enhanced CT and 18F-FDG PET/CT. Further research and assessment are warranted to fully establish the clinical utility of 68Ga-PSMA-11 PET/CT in ccRCC.
准确预测术前不良病理对肾细胞癌(RCC)的治疗计划至关重要。先前的研究强调了前列腺特异性膜抗原正电子发射断层扫描/计算机断层扫描(PSMA PET/CT)在区分良性和恶性局限性肾肿瘤方面的潜力。然而,很少有病例报告阐明了使用 PET/CT 识别侵袭性病理特征的情况。我们的研究旨在前瞻性比较增强 CT、68Ga-PSMA-11 和 18F-氟脱氧葡萄糖(18F-FDG)PET/CT 在伴有坏死或肉瘤样或横纹肌样分化的透明细胞肾细胞癌(ccRCC)中的诊断价值。
纳入了一组接受新诊断的肾肿块患者的前瞻性病例系列,这些患者在肾切除术 30 天内接受了增强 CT、68Ga-PSMA-11 和 18F-FDG PET/CT 检查。记录了完整的术前和术后临床病理数据。排除了接受新辅助靶向治疗、拒绝增强 CT 或 PET/CT 扫描、拒绝手术治疗或具有非 ccRCC 病理指征的患者。在病理特征的亚组内比较了影像学参数。使用 Bonferroni 校正进行多重检验调整,统计学意义设定为 p 值小于 0.017。
72 例患者最终纳入分析。增强 CT 在识别坏死、肉瘤样或横纹肌样分化和不良病理方面表现不佳(均 P > 0.05)。68Ga-PSMA-11 PET/CT 的最大标准化摄取值(SUVmax)在识别肿瘤坏死和不良病理方面优于 18F-FDG PET/CT,曲线下面积(AUC)为 0.85(截断值=25.26,p<0.001;Delong 检验 z=2.709,p=0.007)用于肿瘤坏死和 AUC 为 0.90(截断值=25.26,p<0.001;Delong 检验 z=3.433,p<0.001)用于不良病理。然而,68Ga-PSMA-11 和 18F-FDG PET/CT 在预测肉瘤样或横纹肌样特征方面没有显著的统计学差异(AUC 为 0.91 与 0.75,Delong 检验 z=1.998,p=0.046)。基于年龄、性别、肿瘤位置、最大直径、分期和世卫组织/国际泌尿病理学会分级的亚组分析表明,68Ga-PSMA-11 PET/CT SUVmax 对不良病理具有显著的预测价值。增强 CT 值和 SUVmax 表现出很强的可靠性[组内相关系数(ICC)>0.80],表明相关性很强。
与增强 CT 和 18F-FDG PET/CT 相比,68Ga-PSMA-11 PET/CT 在识别原发性 ccRCC 的侵袭性病理特征方面具有明显优势。需要进一步研究和评估,以充分确定 68Ga-PSMA-11 PET/CT 在 ccRCC 中的临床应用价值。