Guilhaumou Romain, Chevrier Constance, Setti Jean Loup, Jouve Elisabeth, Marsot Amélie, Julian Nathan, Blin Olivier, Simeone Pierre, Lagier David, Mokart Djamel, Bruder Nicolas, Garnier Marc, Velly Lionel
Department of Clinical Pharmacology and Pharmacosurveillance, La Timone University Hospital; 13005 Marseille, France.
Institut de Neurosciences des Systèmes, Aix Marseille University, INSERM UMR 1106, 13005 Marseille, France.
Antibiotics (Basel). 2023 Aug 5;12(8):1289. doi: 10.3390/antibiotics12081289.
The aims of this study were to describe pharmacokinetic/pharmacodynamic target attainment in intensive care unit (ICU) patients treated with continuously infused -lactam antibiotics, their associated covariates, and the impact of dosage adjustment.
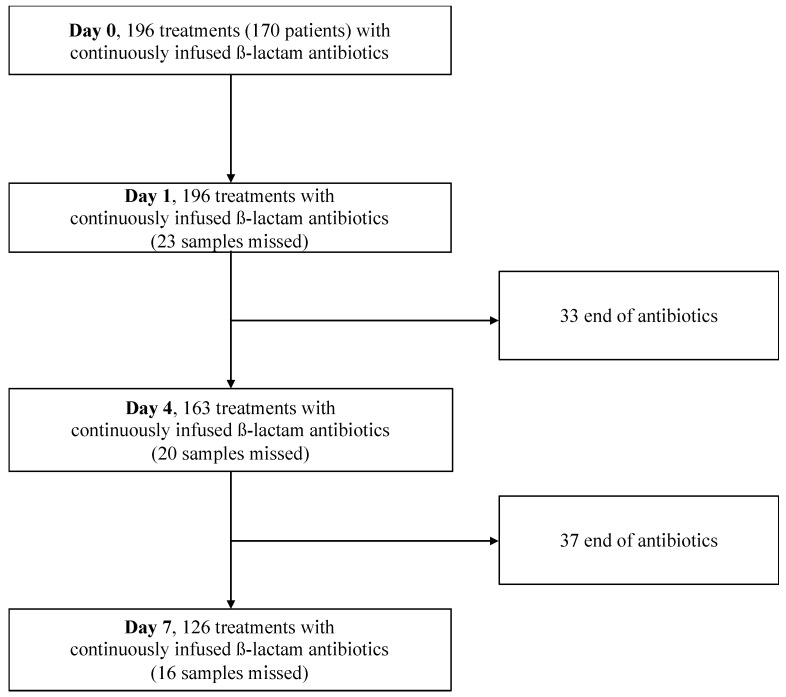
This prospective, observational, cohort study was performed in three ICUs. Four -lactams were continuously infused, and therapeutic drug monitoring (TDM) was performed at days 1, 4, and 7. The primary pharmacokinetic/pharmacodynamic target was an unbound -lactam plasma concentration four times above the bacteria's minimal inhibitory concentration during the whole dosing interval. The demographic and clinical covariates associated with target attainment were evaluated.
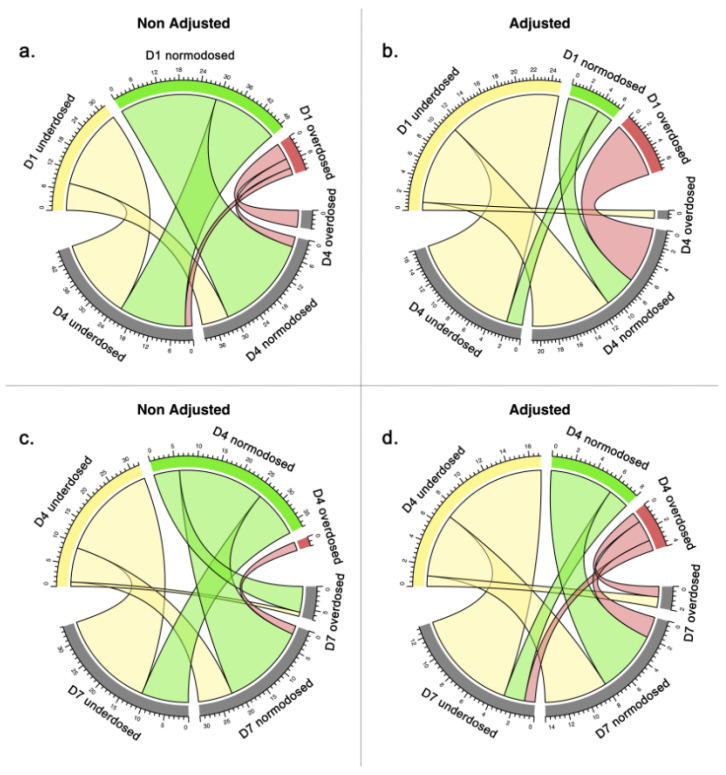
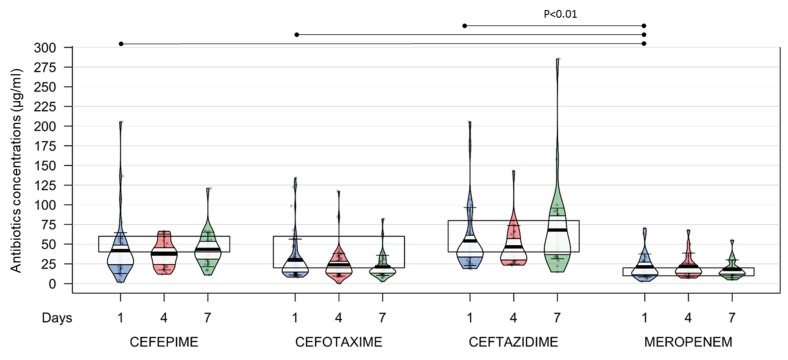
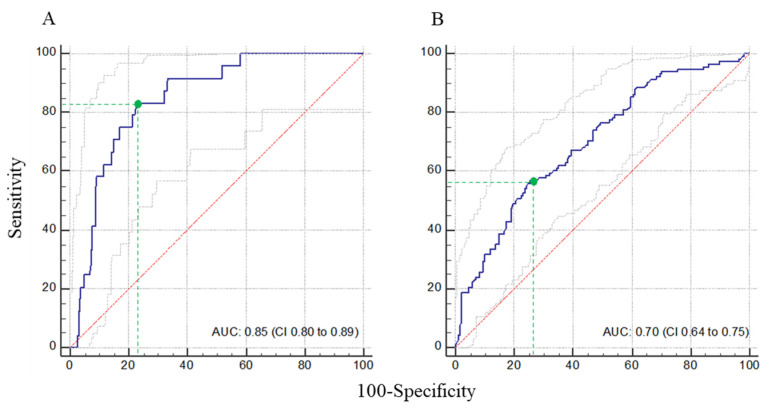
A total of 170 patients were included (426 blood samples). The percentages of empirical -lactam underdosing at D1 were 66% for cefepime, 43% for cefotaxime, 47% for ceftazidime, and 14% for meropenem. Indexed creatinine clearance was independently associated with treatment underdose if increased (adjusted odds ratio per unit, 1.01; 95% CI, 1.00 to 1.01; = 0.014) or overdose if decreased (adjusted odds ratio per unit, 0.95; 95% CI, 0.94 to 0.97; < 0.001). Pharmacokinetic/pharmacodynamic target attainment was significantly increased after -lactam dosage adjustment between day 1 and day 4 vs. no adjustment (53.1% vs. 26.2%; = 0.018).
This study increases our knowledge on the optimization of -lactam therapy in ICU patients. A large inter- and intra-patient variability in plasmatic concentrations was observed, leading to inadequate exposure. A combined indexed creatinine clearance and TDM approach enables adequate dosing for better pharmacokinetic/pharmacodynamic target attainment.
本研究的目的是描述在接受持续输注β-内酰胺类抗生素治疗的重症监护病房(ICU)患者中,药代动力学/药效学目标的达成情况、其相关协变量以及剂量调整的影响。
这项前瞻性、观察性队列研究在三个ICU中进行。四种β-内酰胺类药物持续输注,并在第1天、第4天和第7天进行治疗药物监测(TDM)。主要药代动力学/药效学目标是在整个给药间隔期间,游离β-内酰胺血浆浓度高于细菌最低抑菌浓度四倍。评估与目标达成相关的人口统计学和临床协变量。
共纳入170例患者(426份血样)。第1天经验性β-内酰胺类药物剂量不足的百分比,头孢吡肟为66%,头孢噻肟为43%,头孢他啶为47%,美罗培南为14%。如果升高,校正肌酐清除率指数与治疗剂量不足独立相关(每单位校正比值比,1.01;95%置信区间,1.00至1.01;P = 0.014);如果降低,则与过量独立相关(每单位校正比值比,0.95;95%置信区间,0.94至0.97;P < 0.001)。与第1天至第4天未调整剂量相比,β-内酰胺类药物剂量调整后药代动力学/药效学目标达成率显著提高(53.1%对26.2%;P = 0.018)。
本研究增加了我们对ICU患者β-内酰胺类治疗优化的认识。观察到患者间和患者内血浆浓度存在很大差异,导致暴露不足。联合使用校正肌酐清除率指数和TDM方法能够实现适当给药,以更好地达成药代动力学/药效学目标。