Xue Yuting, Yang Nan, Gu Xunke, Wang Yongqing, Zhang Hua, Jia Keke
Department of Laboratory Medicine, Peking University Third Hospital, Beijing 100191, China.
Department of Blood Transfusion, Peking University Third Hospital, Beijing 100191, China.
Life (Basel). 2023 Jul 28;13(8):1648. doi: 10.3390/life13081648.
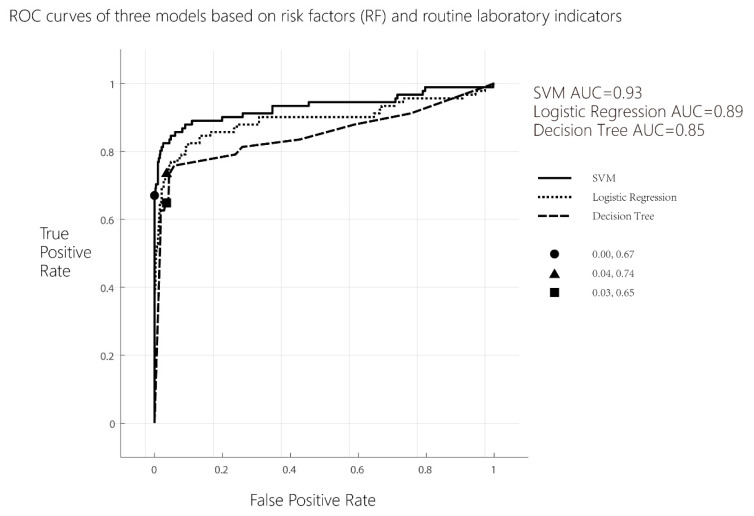
Globally, 10-15% of maternal deaths are statistically attributable to preeclampsia. Compared with late-onset PE, the severity of early-onset PE remains more harmful with higher morbidity and mortality. To establish an early-onset preeclampsia prediction model by clinical characteristics, risk factors and routine laboratory indicators were investigated from pregnant women at 6 to 10 gestational weeks. The clinical characteristics, risk factors, and 38 routine laboratory indicators (6-10 weeks of gestation) including blood lipids, liver and kidney function, coagulation, blood count, and other indicators of 91 early-onset preeclampsia patients and 709 normal controls without early-onset preeclampsia from January 2010 to May 2021 in Peking University Third Hospital (PUTH) were retrospectively analyzed. A logistic regression, decision tree model, and support vector machine (SVM) model were applied for establishing prediction models, respectively. ROC curves were drawn; area under curve (AUC), sensitivity, and specificity were calculated and compared. There were statistically significant differences in the rates of diabetes, antiphospholipid syndrome (APS), kidney disease, obstructive sleep apnea (OSAHS), primipara, history of preeclampsia, and assisted reproductive technology (ART) ( < 0.05). Among the 38 routine laboratory indicators, there were no significant differences in the levels of PLT/LYM, NEU/LYM, TT, D-Dimer, FDP, TBA, ALP, TP, ALB, GLB, UREA, Cr, P, Cystatin C, HDL-C, Apo-A, and Lp(a) between the two groups ( > 0.05). The levels of the rest indicators were all statistically different between the two groups ( < 0.05). If only 12 risk factors of PE were analyzed with the logistic regression, decision tree model, and support vector machine (SVM), and the AUC were 0.78, 0.74, and 0.66, respectively, while 12 risk factors of PE and 38 routine laboratory indicators were analyzed with the logistic regression, decision tree model, and support vector machine (SVM), and the AUC were 0.86, 0.77, and 0.93, respectively. The efficacy of clinical risk factors alone in predicting early-onset preeclampsia is not high while the efficacy increased significantly when PE risk factors combined with routine laboratory indicators. The SVM model was better than logistic regression model and decision tree model in early prediction of early-onset preeclampsia incidence.
在全球范围内,经统计,10%-15%的孕产妇死亡归因于子痫前期。与晚发型子痫前期相比,早发型子痫前期的严重程度更高,发病率和死亡率也更高,危害更大。为通过临床特征建立早发型子痫前期预测模型,对妊娠6至10周的孕妇的危险因素和常规实验室指标进行了调查。回顾性分析了2010年1月至2021年5月在北京大学第三医院(北医三院)就诊的91例早发型子痫前期患者和709例无早发型子痫前期的正常对照的临床特征、危险因素以及38项常规实验室指标(妊娠6-10周),这些指标包括血脂、肝肾功能、凝血、血常规等。分别应用逻辑回归、决策树模型和支持向量机(SVM)模型建立预测模型。绘制ROC曲线;计算并比较曲线下面积(AUC)、敏感性和特异性。糖尿病、抗磷脂综合征(APS)、肾脏疾病、阻塞性睡眠呼吸暂停(OSAHS)、初产妇、子痫前期病史和辅助生殖技术(ART)的发生率存在统计学显著差异(<0.05)。在38项常规实验室指标中,两组间血小板/淋巴细胞比值(PLT/LYM)、中性粒细胞/淋巴细胞比值(NEU/LYM)、凝血酶时间(TT)、D-二聚体、纤维蛋白降解产物(FDP)、总胆汁酸(TBA)、碱性磷酸酶(ALP)、总蛋白(TP)、白蛋白(ALB)、球蛋白(GLB)、尿素(UREA)、肌酐(Cr)、磷(P)、胱抑素C、高密度脂蛋白胆固醇(HDL-C)、载脂蛋白A(Apo-A)和脂蛋白(a)[Lp(a)]水平无显著差异(>0.05)。其余指标水平在两组间均有统计学差异(<0.05)。若仅用逻辑回归、决策树模型和支持向量机(SVM)分析12项子痫前期危险因素,其AUC分别为0.78、0.74和0.66,而用逻辑回归、决策树模型和支持向量机(SVM)分析12项子痫前期危险因素和38项常规实验室指标时,其AUC分别为0.86、0.77和0.93。单独的临床危险因素预测早发型子痫前期的效能不高,而子痫前期危险因素与常规实验室指标联合时效能显著提高。在早发型子痫前期发病的早期预测中,支持向量机(SVM)模型优于逻辑回归模型和决策树模型。