AlAshqar Abdelrahman, Ghazarian Maddie, Webster Emily M, Upadhyay Animesh, Azodi Masoud, Schwartz Peter E, Ratner Elena, Altwerger Gary
Department of Obstetrics, Gynecology and Reproductive Sciences, Yale School of Medicine, New Haven, CT, United States.
Gynecol Oncol Rep. 2023 Jul 10;49:101240. doi: 10.1016/j.gore.2023.101240. eCollection 2023 Oct.
To describe the surgical and oncologic outcomes in surgically treated oldest old women (≥80 years) with endometrioid endometrial cancer as a function of their comorbidities.
In this retrospective cohort study, patients aged 80-99 years who underwent surgical management of stage I endometrioid endometrial cancer between 2006 and 2018 were included. Low- and high-intermediate risk disease was defined using the Gynecologic Oncology Group-99 criteria. The validated, Combined Age-Charlson Comorbidity Index (CA-CCI) was used to quantify comorbidity burden. Logistic regression was used to identify the independent predictors of various surgical and oncologic outcomes. Kaplan-Meier survival analysis was performed to compare survival distributions based on mortality cause and comorbidity status.
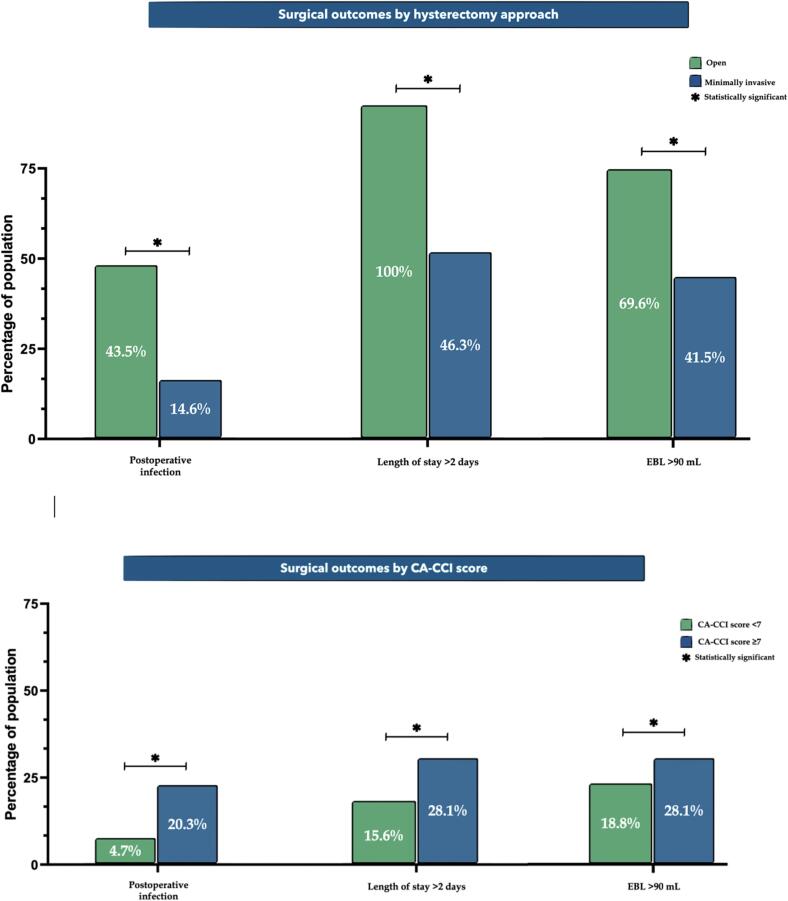
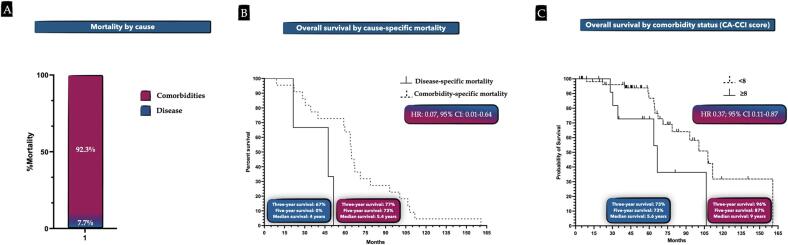
We identified 64 women who met the eligibility criteria. Median age was 84 years (IQR 80, 94 years). Among oldest old women undergoing a hysterectomy with or without lymph node dissection, women with a CA-CCI score of ≥7 had an 8 times higher risk of postoperative infections compared with oldest old women with a <7 score (95% CI 1.53-48.91, = 0.015). Women with a CA-CCI score of ≥8 were 45% less likely to survive at 3 years (aRR 0.55, 95% CI 0.004-0.87; = 0.039) than those with a lower CA-CCI score (three-year overall survival 73% vs 96%).
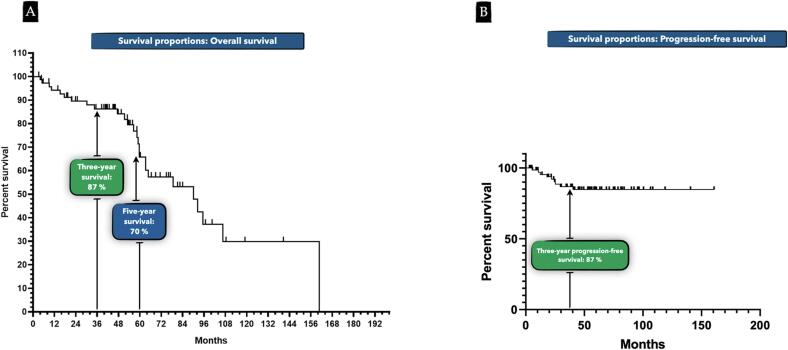
Surgical and oncologic outcomes in oldest old women with early stage endometrioid endometrial cancer are largely determined by comorbidity status. Less comorbid women (CA-CCI score < 8) had a significantly higher five-year survival at 87% than their more comorbid counterparts. Use of age-comorbidity risk scoring such as CA-CCI, preoperative optimization, and careful selection for and counseling of patients about surgical treatment are paramount in providing optimal recovery and survival advantages in the oldest old.
描述手术治疗的高龄老年女性(≥80岁)子宫内膜样腺癌患者的手术及肿瘤学结局,并分析其与合并症的关系。
在这项回顾性队列研究中,纳入了2006年至2018年间接受I期子宫内膜样腺癌手术治疗的80 - 99岁患者。低、中高风险疾病采用妇科肿瘤学组-99标准定义。使用经过验证的联合年龄-查尔森合并症指数(CA-CCI)来量化合并症负担。采用逻辑回归分析确定各种手术及肿瘤学结局的独立预测因素。进行Kaplan-Meier生存分析,以比较基于死亡原因和合并症状态的生存分布情况。
我们确定了64名符合纳入标准的女性。中位年龄为84岁(四分位间距80,94岁)。在接受子宫切除术(无论是否行淋巴结清扫)的高龄老年女性中,CA-CCI评分≥7的女性术后感染风险是CA-CCI评分<7的女性的8倍(95%可信区间1.53 - 48.91,P = 0.015)。CA-CCI评分≥8的女性3年生存率比CA-CCI评分较低的女性低45%(调整后风险比0.55,95%可信区间0.004 - 0.87;P = 0.039)(三年总生存率分别为73%和96%)。
早期子宫内膜样腺癌高龄老年女性的手术及肿瘤学结局在很大程度上取决于合并症状态。合并症较少的女性(CA-CCI评分<8)五年生存率显著更高,为87%,高于合并症较多的女性。使用如CA-CCI这样的年龄-合并症风险评分、术前优化以及对患者进行仔细的手术治疗选择和咨询,对于高龄老年患者实现最佳恢复和生存优势至关重要。