Department of Medicine, Division of Cardiology, Centre for Cardiovascular Innovation and Cardiovascular Imaging Research Core Laboratory (CIRCL), University of British Columbia, Rm 9111, 2775 Laurel Street, Vancouver, BC V5Z 1M9, Canada.
Department of Medicine, Division of General Internal Medicine, Centre for Heart and Lung Innovation, University of British Columbia, Vancouver, BC, Canada.
Eur Heart J. 2024 Jan 7;45(2):117-128. doi: 10.1093/eurheartj/ehad539.
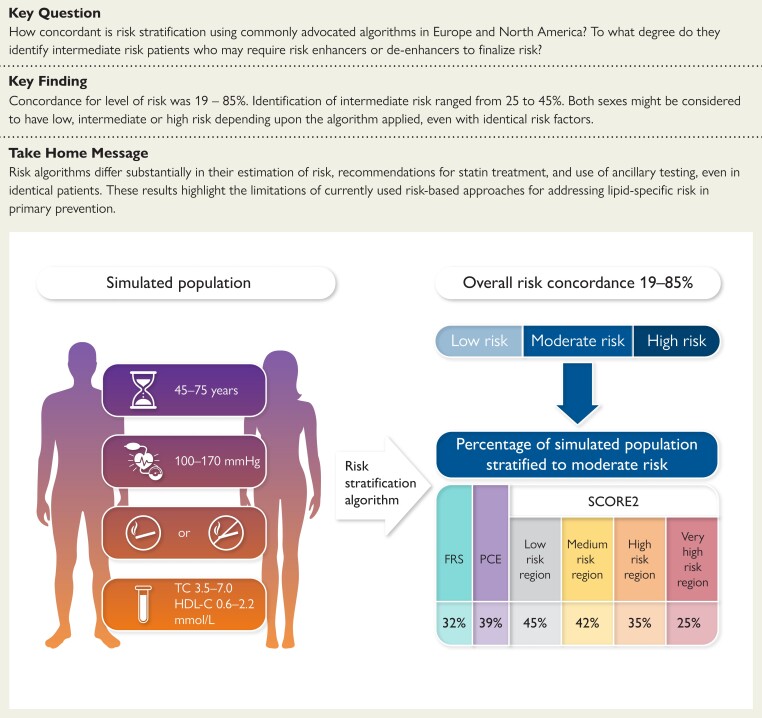
Statin recommendations in primary prevention depend upon risk algorithms. Moreover, with intermediate risk, risk enhancers and de-enhancers are advocated to aid decisions. The aim of this study was to compare algorithms used in North America and Europe for the identification of patients warranting statin or consideration of risk enhancers and de-enhancers.
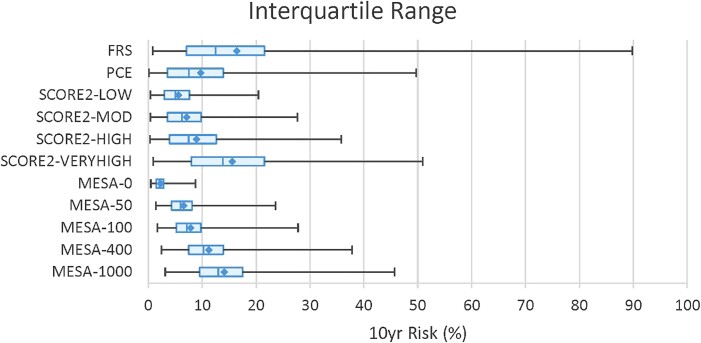
A simulated population (n = 7680) equal in males and females, with/without smoking, aged 45-70 years, total cholesterol 3.5-7.0 mmol/L, high-density lipoprotein cholesterol 0.6-2.2 mmol/L, and systolic blood pressure 100-170 mmHg, was evaluated. High, intermediate, and low risks were determined using the Framingham Risk Score (FRS), Pooled Cohort Equation (PCE), four versions of Systematic Coronary Risk Evaluation 2 (SCORE2), and Multi-Ethnic Study of Atherosclerosis (MESA) algorithm (0-1000 Agatston Units).
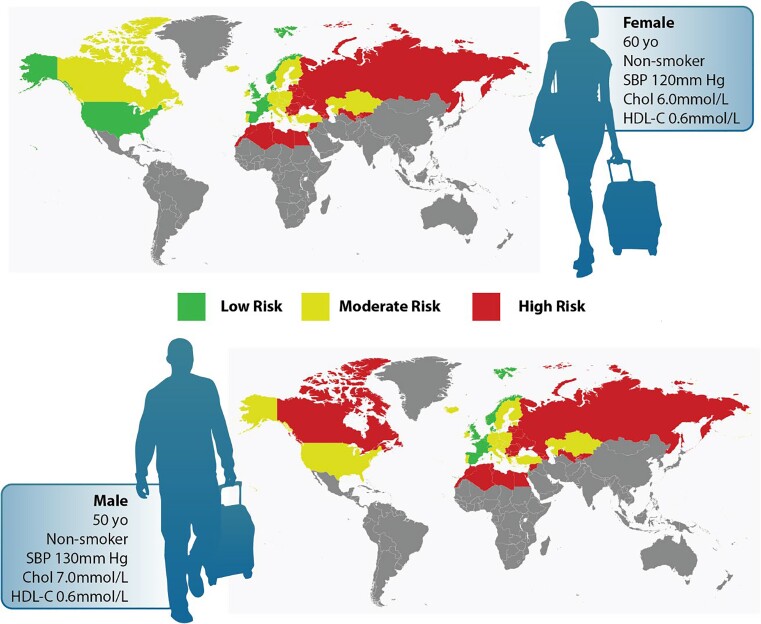
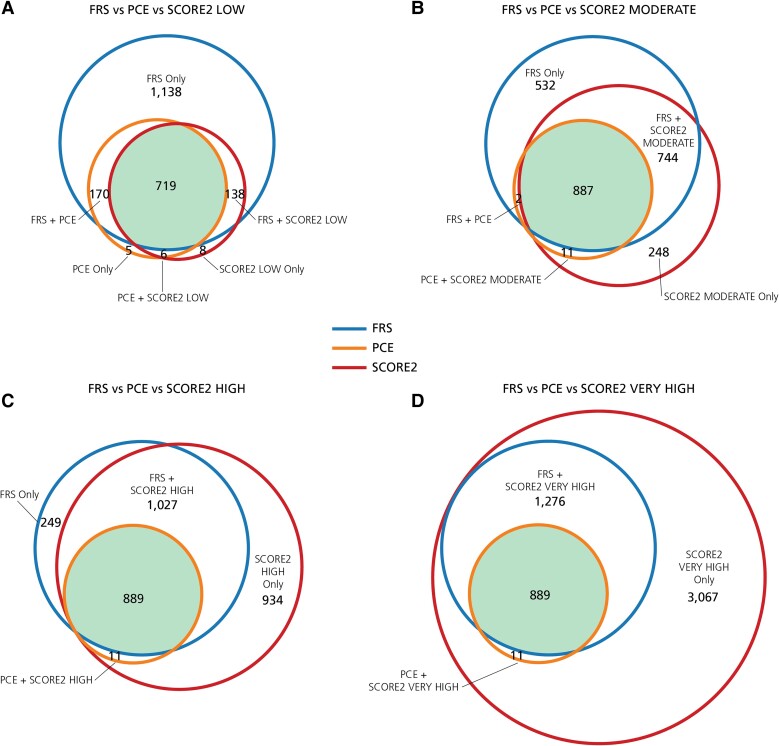
Concordance for the three levels of risk varied from 19% to 85%. Both sexes might be considered to have low, intermediate, or high risk depending on the algorithm applied, even with the same burden of risk factors. Only SCORE2 (High Risk and Very High Risk versions) identified equal proportions of males and females with high risk. Excluding MESA, the proportion with moderate risk was 25% (SCORE2, Very High Risk Region), 32% (FRS), 39% (PCE), and 45% (SCORE2, Low Risk Region).
Risk algorithms differ substantially in their estimation of risk, recommendations for statin treatment, and use of ancillary testing, even in identical patients. These results highlight the limitations of currently used risk-based approaches for addressing lipid-specific risk in primary prevention.
他汀类药物在一级预防中的推荐取决于风险算法。此外,对于中危人群,建议使用风险增强和减弱因素来辅助决策。本研究的目的是比较北美和欧洲用于识别需要他汀类药物治疗或考虑使用风险增强和减弱因素的患者的算法。
模拟了一个性别比例相等(男性和女性各占 50%)、有/无吸烟史、年龄在 45-70 岁、总胆固醇在 3.5-7.0mmol/L、高密度脂蛋白胆固醇在 0.6-2.2mmol/L、收缩压在 100-170mmHg 的人群(n=7680)。使用 Framingham 风险评分(FRS)、Pooled Cohort Equation(PCE)、四种版本的 Systematic Coronary Risk Evaluation 2(SCORE2)和 Multi-Ethnic Study of Atherosclerosis(MESA)算法(0-1000AgatstonUnits)来确定高、中、低风险。
三种风险水平的一致性在 19%-85%之间。即使危险因素负担相同,不同的算法也可能导致男性和女性被认为具有低、中或高风险。只有 SCORE2(高风险和极高风险版本)可以识别出相同比例的男性和女性具有高风险。不包括 MESA,中度风险的比例分别为 SCORE2(极高风险区)25%、FRS32%、PCE39%和 SCORE2(低风险区)45%。
即使在相同的患者中,风险算法在风险估计、他汀类药物治疗建议和辅助检测的使用方面也存在显著差异。这些结果强调了目前基于风险的方法在解决一级预防中特定于脂质的风险方面的局限性。