Mancini G B John, Ryomoto Arnold
Division of Cardiology, Department of Medicine, Centre for Cardiovascular Innovation, University of British Columbia, Vancouver, British Columbia, Canada.
JACC Adv. 2024 Jul 18;3(8):101122. doi: 10.1016/j.jacadv.2024.101122. eCollection 2024 Aug.
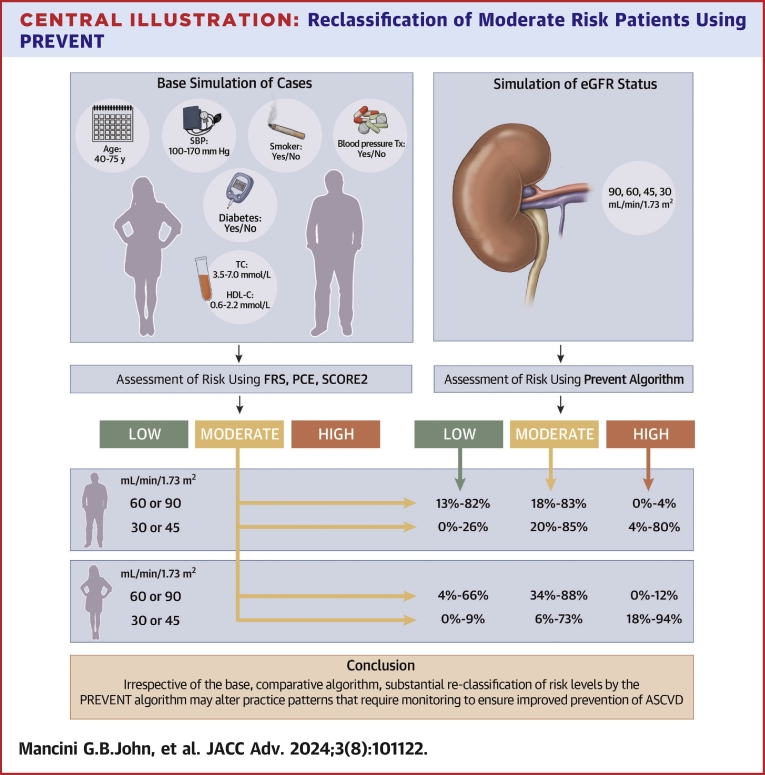
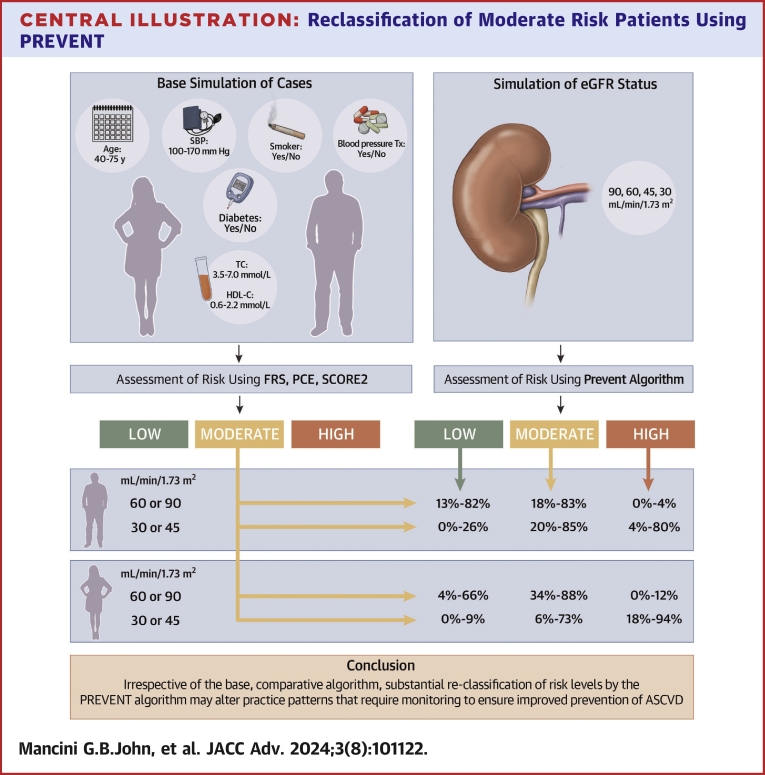
The PREVENT (Predicting Risk of cardiovascular disease EVENTs risk algorithm was developed to better reflect the impact of metabolic factors on cardiovascular risk.
The purpose of this study was to compare the relative performance of PREVENT with standard comparator algorithms (Framingham risk score, pooled cohort equation, SCORE2 [Systematic COronary Risk Evaluation2]) for risk stratification emphasizing the implications of weighing chronic kidney disease.
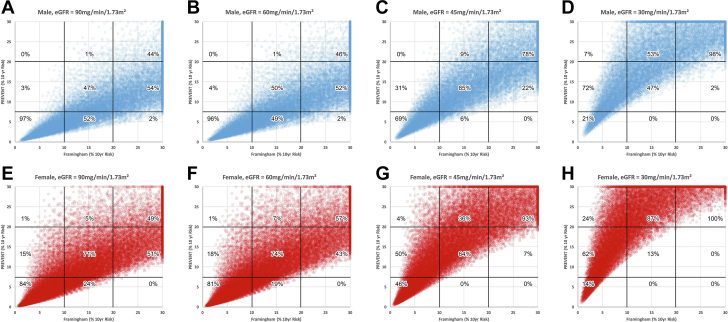
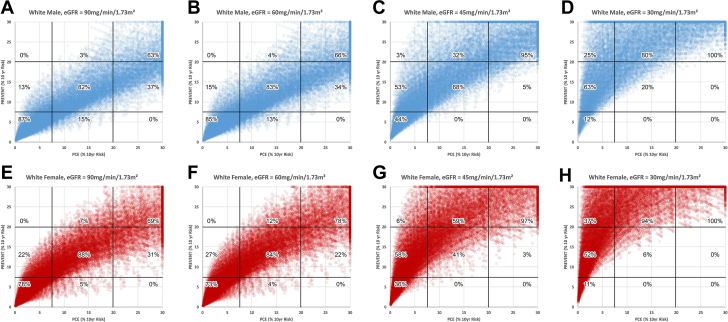
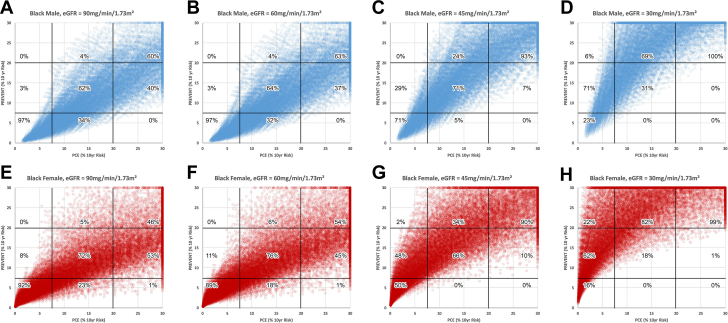
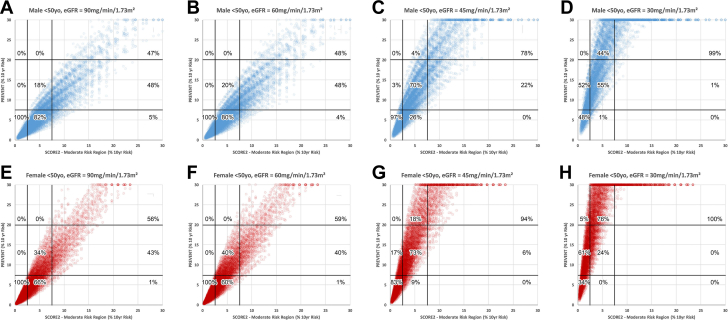
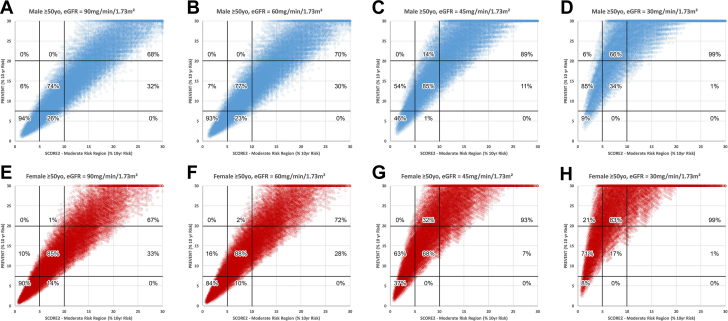
A simulated cohort was created of males and females aged 40 to 75 years with and without other traditional risk factors and either normal estimated glomerular filtration rates (eGFR 90 or 60 ml/min/1.73 m) or abnormal eGFR (45 or 30 ml/min/1.73 m). The concordance and reclassification rates were calculated for each category of risk with emphasis on subjects characterized as moderate risk by the standard comparator algorithms.
PREVENT demonstrated increased risk with progressive decreases in eGFR. When the standard comparator algorithms identified moderate risk, PREVENT was concordant in 6% to 88% of simulations. In simulations with normal eGFR, PREVENT identified a lower risk in 18% to 88% and a higher risk in 0% to 12% of simulations. Conversely, with abnormal eGFR, PREVENT identified lower risk in 0% to 26% and higher risk in 4% to 94% of simulations.
PREVENT substantially reclassifies risk and has the potential to alter prevention practice patterns. The tendency to assign a lower risk compared to standard algorithms when eGFR is normal may diminish implementation of preventive therapy. National health care systems need to monitor whether such changes improve overall public health.
开发了PREVENT(预测心血管疾病事件风险算法)以更好地反映代谢因素对心血管风险的影响。
本研究的目的是比较PREVENT与标准对照算法(弗雷明汉风险评分、合并队列方程、SCORE2[系统性冠状动脉风险评估2])在风险分层方面的相对性能,重点强调权衡慢性肾病的影响。
创建了一个模拟队列,其中包括年龄在40至75岁之间、有或没有其他传统风险因素、估计肾小球滤过率(eGFR)正常(90或60ml/min/1.73m²)或异常(45或30ml/min/1.73m²)的男性和女性。计算每个风险类别的一致性和重新分类率,重点关注被标准对照算法判定为中度风险的受试者。
随着eGFR逐渐降低PREVENT显示风险增加。当标准对照算法判定为中度风险时,PREVENT在6%至88%的模拟中与之一致。在eGFR正常的模拟中,PREVENT在18%至88%的模拟中判定风险较低,在0%至12%的模拟中判定风险较高。相反,在eGFR异常的模拟中,PREVENT在0%至26%的模拟中判定风险较低,在4%至94%的模拟中判定风险较高。
PREVENT能显著重新分类风险,并有可能改变预防实践模式。当eGFR正常时,与标准算法相比倾向于判定较低风险可能会减少预防性治疗的实施。国家医疗保健系统需要监测此类变化是否能改善整体公众健康。