Veldwijk Jorien, DiSantostefano Rachael Lynn, Janssen Ellen, Simons Gwenda, Englbrecht Matthias, Schölin Bywall Karin, Radawski Christine, Raza Karim, Hauber Brett, Falahee Marie
School of Health Policy and Management, Erasmus University Rotterdam, P.O. Box 1738, 3000, Rotterdam, The Netherlands.
Erasmus Choice Modelling Centre, Erasmus University Rotterdam, Rotterdam, The Netherlands.
Patient. 2023 Nov;16(6):641-653. doi: 10.1007/s40271-023-00643-w. Epub 2023 Aug 30.
We aimed to empirically compare maximum acceptable risk results estimated using both a discrete choice experiment (DCE) and a probabilistic threshold technique (PTT).
Members of the UK general public (n = 982) completed an online survey including a DCE and a PTT (in random order) measuring their preferences for preventative treatment for rheumatoid arthritis. For the DCE, a Bayesian D-efficient design consisting of four blocks of 15 choice tasks was constructed including six attributes with varying levels. The PTT used identical risk and benefit attributes. For the DCE, a panel mixed-logit model was conducted, both mean and individual estimates were used to calculate maximum acceptable risk. For the PTT, interval regression was used to calculate maximum acceptable risk. Perceived complexity of the choice tasks and preference heterogeneity were investigated for both methods.
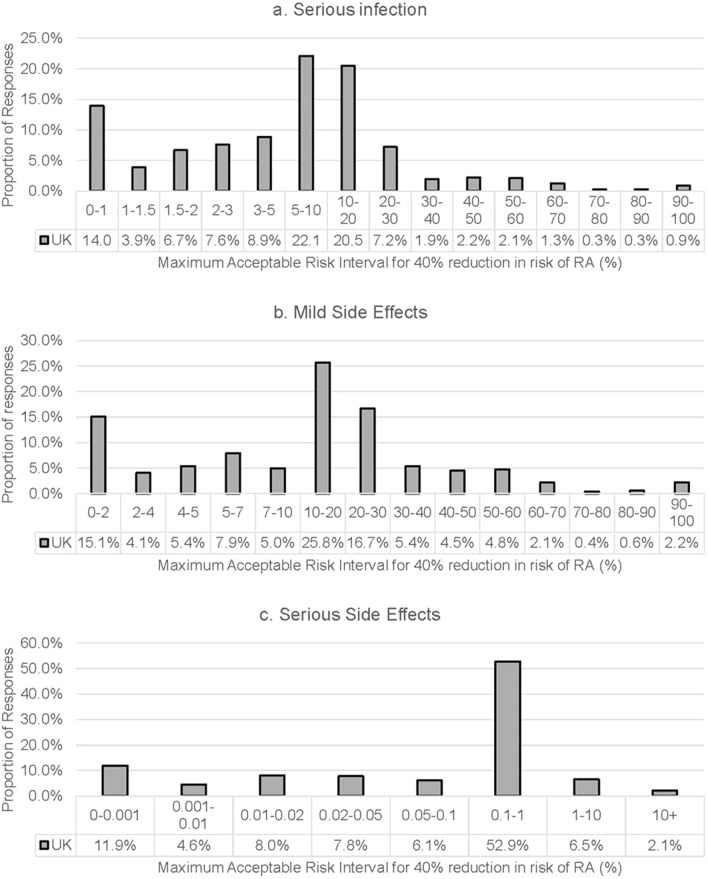
Maximum acceptable risk confidence intervals of both methods overlapped for serious infection and serious side effects but not for mild side effects (maximum acceptable risk was 32.7 percent-points lower in the PTT). Although, both DCE and PTT tasks overall were considered easy or very easy to understand and answer, significantly more respondents rated the DCE choice tasks as easier to understand compared with those who rated the PTT as easier (7-percentage point difference; p < 0.05).
Maximum acceptable risk estimate confidence intervals based on a DCE and a PTT overlapped for two out of the three included risk attributes. More respondents rated the DCE as easier to understand. This may suggest that the DCE is better suited in studies estimating maximum acceptable risk for multiple risk attributes of differing severity, while the PTT may be better suited when measuring heterogeneity in maximum acceptable risk estimates or when investigating one or more serious adverse events.
我们旨在通过实证比较使用离散选择实验(DCE)和概率阈值技术(PTT)估计的最大可接受风险结果。
英国公众成员(n = 982)完成了一项在线调查,其中包括一个DCE和一个PTT(顺序随机),以测量他们对类风湿性关节炎预防性治疗的偏好。对于DCE,构建了一个由四个包含15个选择任务的模块组成的贝叶斯D效率设计,包括六个具有不同水平的属性。PTT使用相同的风险和收益属性。对于DCE,进行了面板混合逻辑模型分析,使用均值和个体估计值来计算最大可接受风险。对于PTT,使用区间回归来计算最大可接受风险。研究了两种方法中选择任务的感知复杂性和偏好异质性。
两种方法对于严重感染和严重副作用的最大可接受风险置信区间重叠,但对于轻度副作用不重叠(PTT中的最大可接受风险低32.7个百分点)。尽管DCE和PTT任务总体上被认为易于理解和回答,但与认为PTT更易于理解的受访者相比,显著更多的受访者认为DCE选择任务更易于理解(相差7个百分点;p < 0.05)。
基于DCE和PTT的最大可接受风险估计置信区间在三个纳入的风险属性中的两个上重叠。更多受访者认为DCE更易于理解。这可能表明DCE更适合于估计不同严重程度的多个风险属性的最大可接受风险的研究,而PTT可能更适合于测量最大可接受风险估计中的异质性或调查一个或多个严重不良事件时。