School of Medicine, University College Cork, Cork, Ireland.
Department of Physiology, University College Cork, Cork, Ireland.
J Hum Hypertens. 2024 Jan;38(1):29-44. doi: 10.1038/s41371-023-00857-3. Epub 2023 Sep 4.
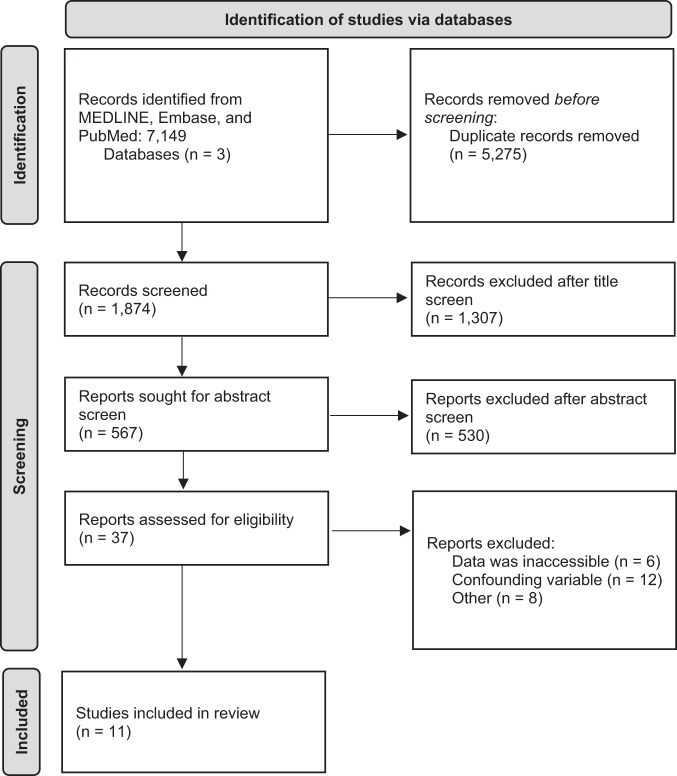
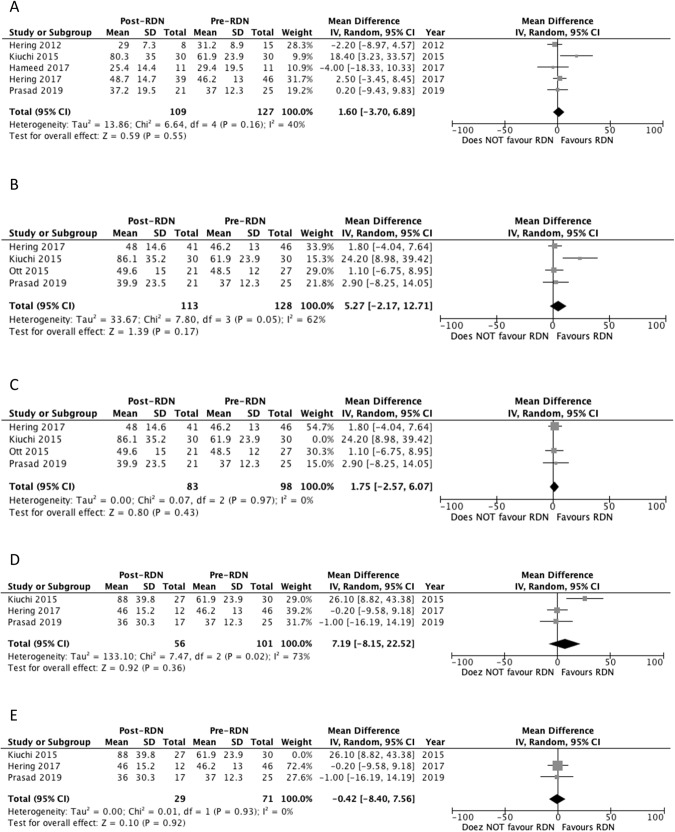
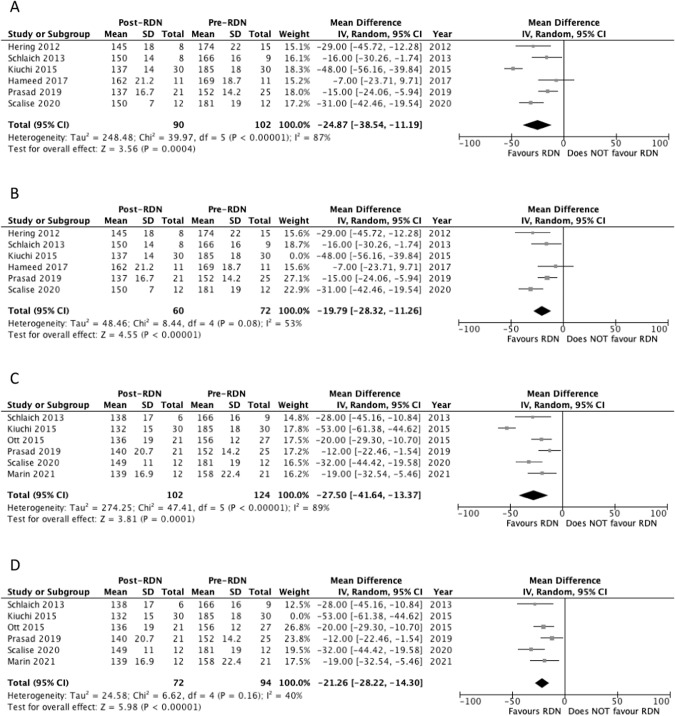
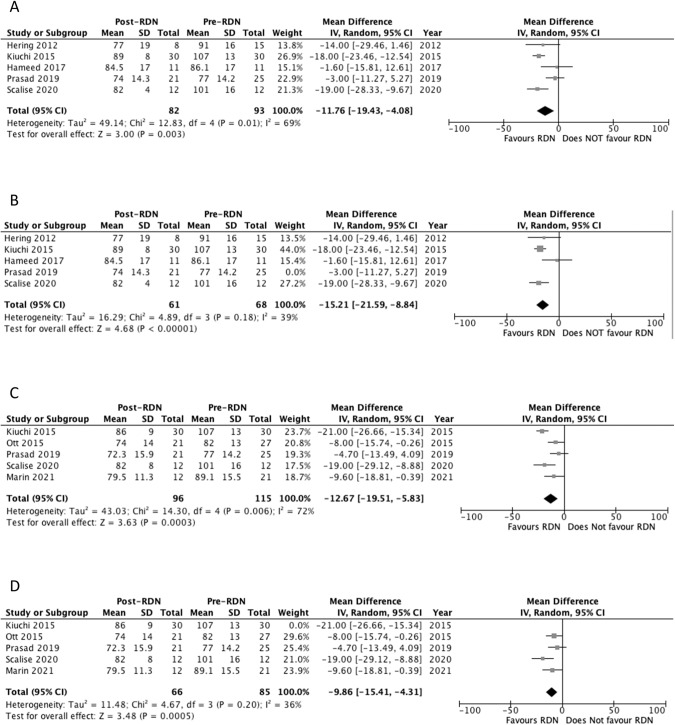
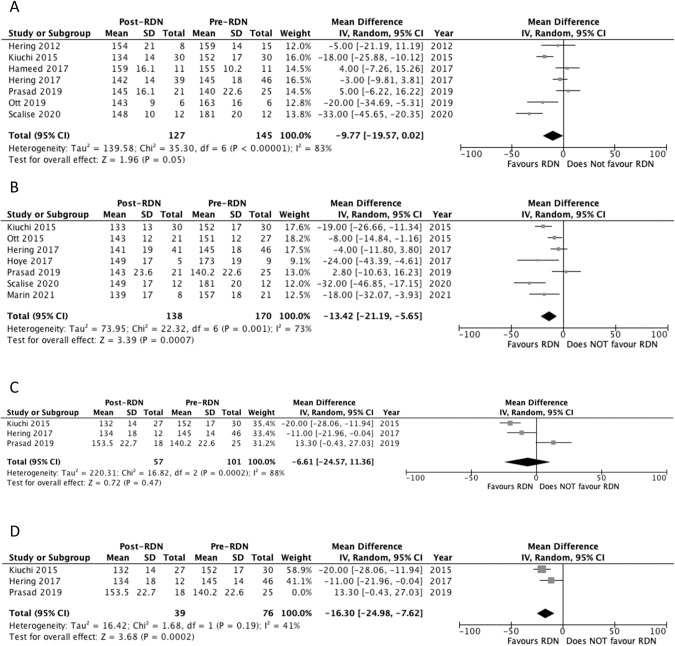
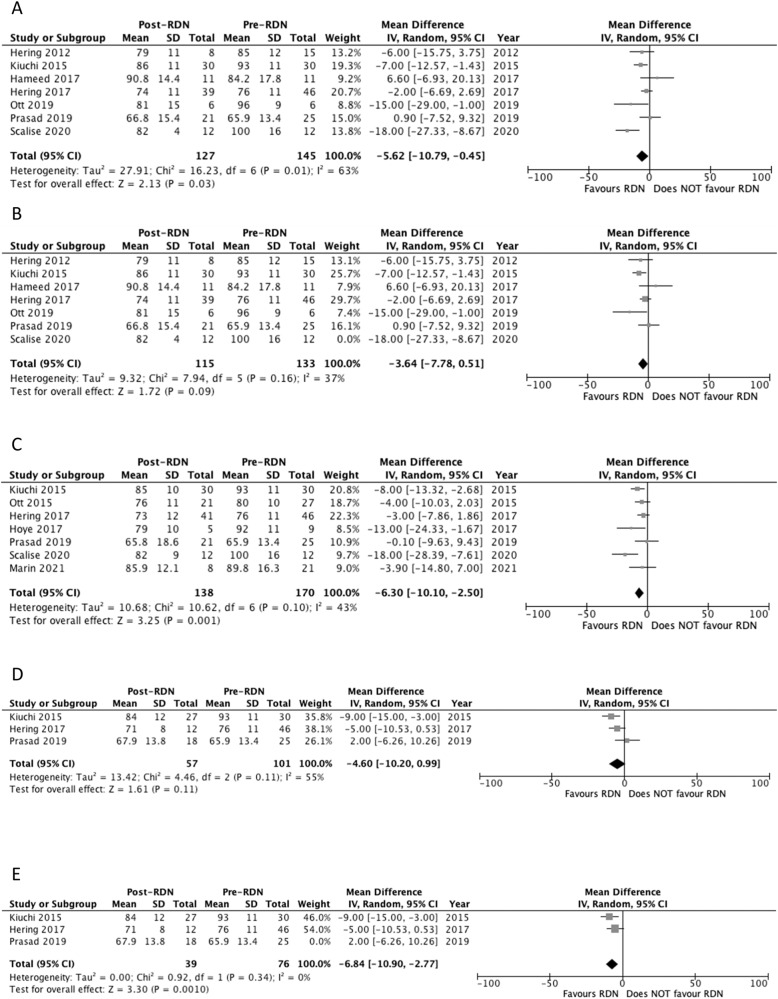
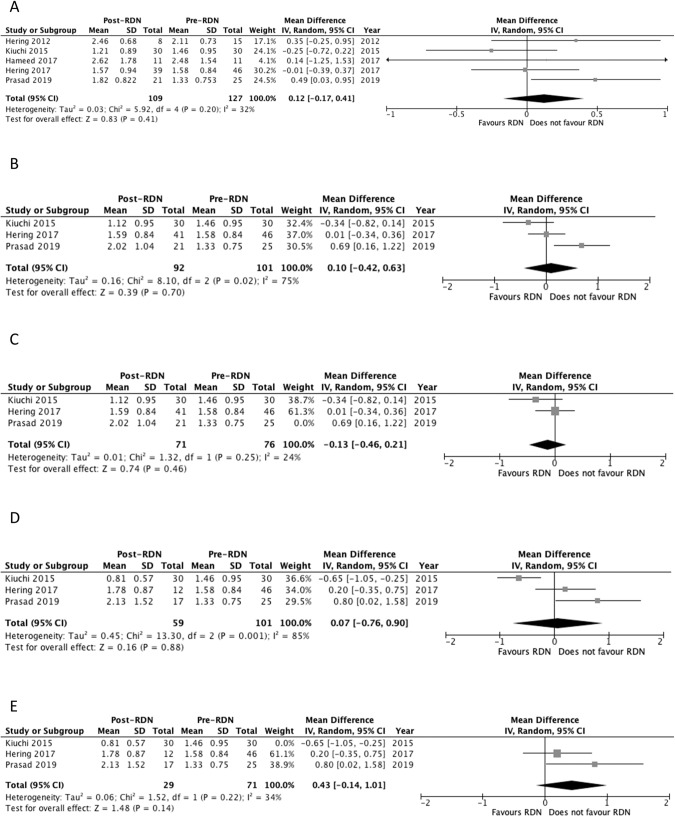
The present study aims to evaluate the clinical outcomes following renal denervation (RDN) for hypertensive patients with chronic kidney disease (CKD). Prospective studies published between January 1, 2010 and November 15, 2022 where systematically identified for RDN outcomes on office and ambulatory blood pressure, estimated glomerular filtration rate (eGFR), creatinine and procedural characteristics from three online databases (Medline, PubMed, EMBASE). Random effects model to combine risk ratios and mean differences was used. Where possible, clinical outcomes were pooled and analyzed at 6, 12 and 24 months. Significance was set at p ≤ 0.05. 11 prospective trials, with a total of 226 patients with treatment resistant HTN receiving RDN met the inclusion criteria. Age ranged from 42.5 ± 13.8 to 66 ± 9. Main findings of this review included a reduction in systolic and diastolic office blood pressure at 6 [-19.8 (p < 0.00001)/-15.2 mm Hg (p < 0.00001)] and 12 months [-21.2 (p < 0.00001)/-9.86 mm Hg (p < 0.0005)] follow-up compared to baseline. This was also seen in systolic and diastolic 24-hour ambulatory blood pressure at 6 [-9.77 (p = 0.05)/-3.64 mm Hg (p = 0.09)] and 12 months [-13.42 (p = 0.0007)/-6.30 mm Hg (p = 0.001)] follow-up compared to baseline. The reduction in systolic and diastolic 24-hour ambulatory blood pressure was maintained to 24 months [(-16.30 (p = 0.0002)/-6.84 mm Hg (p = 0.0010)]. Analysis of kidney function through eGFR demonstrated non-significant results at 6 (+1.60 mL/min/1.73 m, p = 0.55), 12 (+5.27 mL/min/1.73 m, p = 0.17), and 24 months (+7.19 mL/min/1.73 m, p = 0.36) suggesting an interruption in natural CKD progression. Similar results were seen in analysis of serum creatinine at 6 (+0.120 mg/dL, p = 0.41), 12 (+0.100 mg/dL, p = 0.70), and 24 months (+0.07 mg/dL, p = 0.88). Assessment of procedural complications deemed RDN in a CKD cohort to be safe with an overall complication rate of 4.86%. With the current advances in RDN and its utility in multiple chronic diseases beyond hypertension, the current study summarizes critical findings that further substantiate the literature regarding the potential of such an intervention to be incorporated as an effective treatment for resistant hypertension and CKD.
本研究旨在评估肾去神经术(RDN)治疗慢性肾脏病(CKD)合并高血压患者的临床疗效。2010 年 1 月 1 日至 2022 年 11 月 15 日期间,系统地从三个在线数据库(Medline、PubMed、EMBASE)中检索了关于 RDN 对诊室和动态血压、估计肾小球滤过率(eGFR)、肌酐和手术特征的前瞻性研究。使用随机效应模型对风险比和平均差异进行合并。尽可能在 6、12 和 24 个月时对临床结果进行汇总和分析。p 值≤0.05 为有统计学意义。11 项前瞻性试验,共纳入 226 例接受 RDN 治疗的难治性 HTN 患者,符合纳入标准。年龄范围为 42.5±13.8 至 66±9。本综述的主要发现包括治疗后 6 个月[-19.8(p<0.00001)/-15.2mmHg(p<0.00001)]和 12 个月[-21.2(p<0.00001)/-9.86mmHg(p<0.0005)]诊室血压下降,与基线相比。这在 6 个月[-9.77(p=0.05)/-3.64mmHg(p=0.09)]和 12 个月[-13.42(p=0.0007)/-6.30mmHg(p=0.001)]动态血压监测中也得到了观察。与基线相比,24 个月时的收缩压和舒张压 24 小时动态血压下降仍保持稳定[(-16.30(p=0.0002)/-6.84mmHg(p=0.0010)]。通过 eGFR 评估肾功能的结果显示,6 个月时无显著变化(+1.60mL/min/1.73m,p=0.55),12 个月时无显著变化(+5.27mL/min/1.73m,p=0.17),24 个月时无显著变化(+7.19mL/min/1.73m,p=0.36),提示 CKD 自然进展中断。在血清肌酐分析中也得到了相似的结果,6 个月时为(+0.120mg/dL,p=0.41),12 个月时为(+0.100mg/dL,p=0.70),24 个月时为(+0.07mg/dL,p=0.88)。评估手术并发症认为 RDN 在 CKD 患者中是安全的,总并发症发生率为 4.86%。随着 RDN 的当前进展及其在高血压以外的多种慢性疾病中的应用,本研究总结了关键发现,进一步证实了关于此类干预措施的潜在应用的文献,即将其作为治疗难治性高血压和 CKD 的有效治疗方法。