Srichawla Bahadar S, Sivakumar Shravan, Cheraghi Seyedeh N, Kipkorir Vincent, Garcia-Dominguez Maria A
Department of Neurology, University of Massachusetts Chan Medical School, Worcester, MA, USA.
Department of Medicine, University of Nairobi, Nairobi, Kenya.
SAGE Open Med Case Rep. 2023 Sep 1;11:2050313X231198322. doi: 10.1177/2050313X231198322. eCollection 2023.
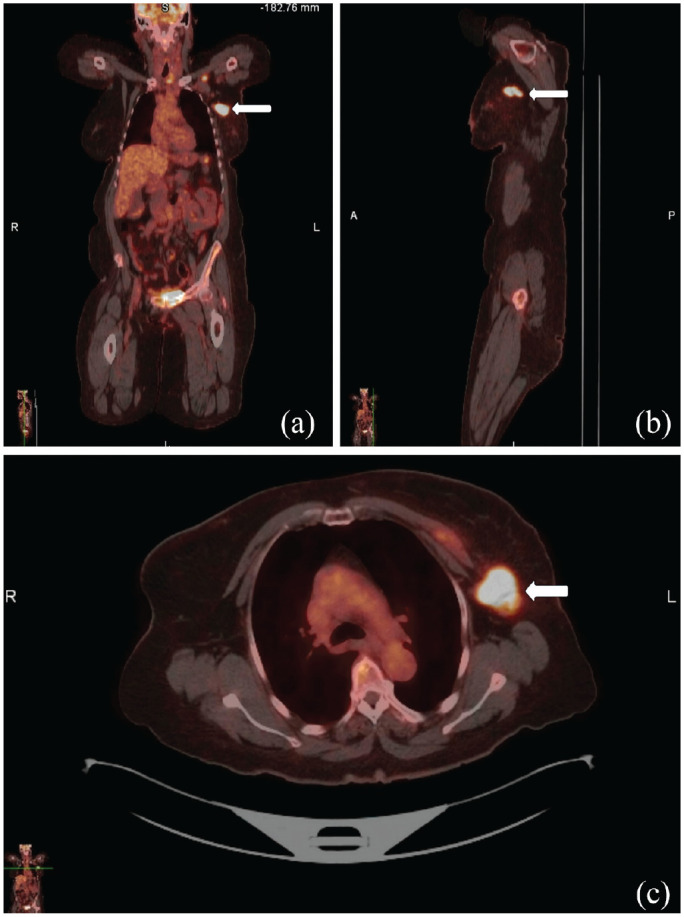
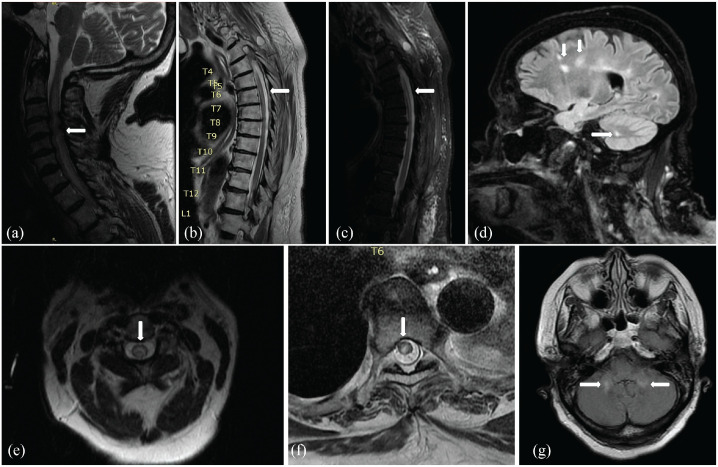
Neuromyelitis optica, an autoimmune inflammatory disorder affecting the central nervous system, can occur in a paraneoplastic context, although rare. We report an intriguing case of a 71-year-old woman with a history of triple-negative infiltrating ductal breast carcinoma, manifesting with paraneoplastic neuromyelitis optica that led to significant respiratory failure and required a cervical laminectomy. The patient presented with pain in the left breast, weakness in the lower extremities, and neck pain. The neurological evaluation showed 2/5 muscle strength in all extremities, diffuse hyperreflexia, and loss of multimodal sensation below the shoulder. She developed acute respiratory failure that required mechanical ventilation. Magnetic resonance imaging highlighted a diffuse abnormal increase in T2 signal intensity throughout the posterior and central portion of the cervical and thoracic spinal cord consistent with longitudinally extensive transverse myelitis, and significant cervical cord compression at C3-C4. Magnetic resonance imaging of the brain showed non-enhancing T2/fluid-attenuated inversion recovery (FLAIR) white matter hyperintensities and cerebellar hemispheres. The serum cell-based assay study demonstrated a high anti-aquaporin-4 immunoglobulin G titer (>1:160) confirming the diagnosis of neuromyelitis optica. She was taken for bilateral laminectomy from C3 to C6. Despite intravenous methylprednisolone and plasmapheresis treatment, no significant recovery was achieved, necessitating tracheostomy and percutaneous endoscopic gastrostomy. Subsequent rituximab treatment led to a mild improvement, with no new lesions on repeat magnetic resonance imaging. This case raises suspicion of the potential for neuromyelitis optica to occur as a paraneoplastic phenomenon, strengthening the need for vigilance in patients with malignancies.
视神经脊髓炎是一种影响中枢神经系统的自身免疫性炎症性疾病,虽罕见,但可发生于副肿瘤性背景下。我们报告了一例71岁女性的有趣病例,该患者有三阴性浸润性导管乳腺癌病史,表现为副肿瘤性视神经脊髓炎,导致严重呼吸衰竭,需要进行颈椎椎板切除术。患者出现左乳疼痛、下肢无力和颈部疼痛。神经学评估显示四肢肌力均为2/5、弥漫性反射亢进以及肩部以下多种感觉丧失。她发展为急性呼吸衰竭,需要机械通气。磁共振成像显示颈段和胸段脊髓后部和中部T2信号强度弥漫性异常增加,符合纵向广泛横贯性脊髓炎,且C3 - C4水平存在明显的颈髓受压。脑部磁共振成像显示非强化的T2/液体衰减反转恢复序列(FLAIR)白质高信号和小脑半球病变。基于血清细胞的检测研究显示抗水通道蛋白4免疫球蛋白G滴度高(>1:160),确诊为视神经脊髓炎。她接受了C3至C6的双侧椎板切除术。尽管进行了静脉注射甲泼尼龙和血浆置换治疗,但未取得显著恢复,因此需要进行气管切开术和经皮内镜下胃造口术。随后的利妥昔单抗治疗带来了轻微改善,复查磁共振成像未见新病灶。该病例引发了对视神经脊髓炎作为副肿瘤现象发生可能性的怀疑,强化了对恶性肿瘤患者保持警惕的必要性。