Kuno Toshiki, Arce Javier, Fattouh Michael, Sarkar Sharmila, Skendelas John P, Daich Jonathan, Schenone Aldo L, Zhang Lili, Rodriguez Carlos J, Virani Salim S, Slomka Piotr J, Shaw Leslee J, Williamson Eric E, Berman Daniel S, Garcia Mario J, Dey Damini, Slipczuk Leandro
Cardiology Division, Montefiore Medical Center, Montefiore Medical Center/Albert Einstein Colalege of Medicine, Cardiology Division. 111 E210th, Bronx, NY 10467, United States.
Cardiothoracic and Vascular Surgery Department, Montefiore Medical Center/Albert Einstein College of Medicine, Bronx, NY, United States.
Am J Prev Cardiol. 2023 Aug 22;15:100578. doi: 10.1016/j.ajpc.2023.100578. eCollection 2023 Sep.
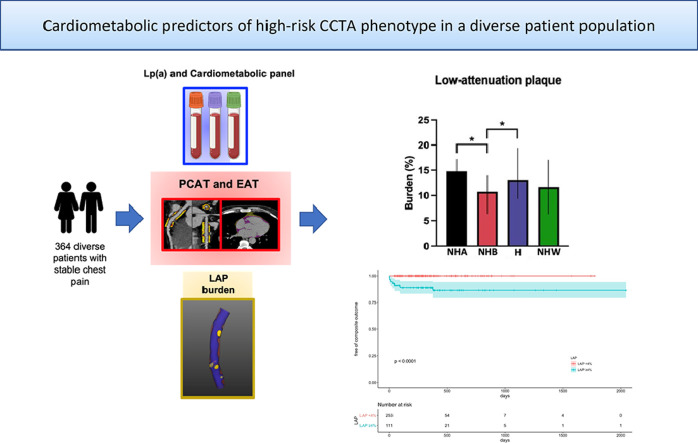
Low-attenuation non-calcified plaque (LAP) burden and vascular inflammation by pericoronary adipose tissue (PCAT) measured from coronary CT angiography (CCTA) have shown to be predictors of cardiovascular outcomes. We aimed to investigate the relationships of cardiometabolic risk factors including lipoprotein(a) and epicardial adipose tissue (EAT) with CCTA high-risk imaging biomarkers, LAP and vascular inflammation.
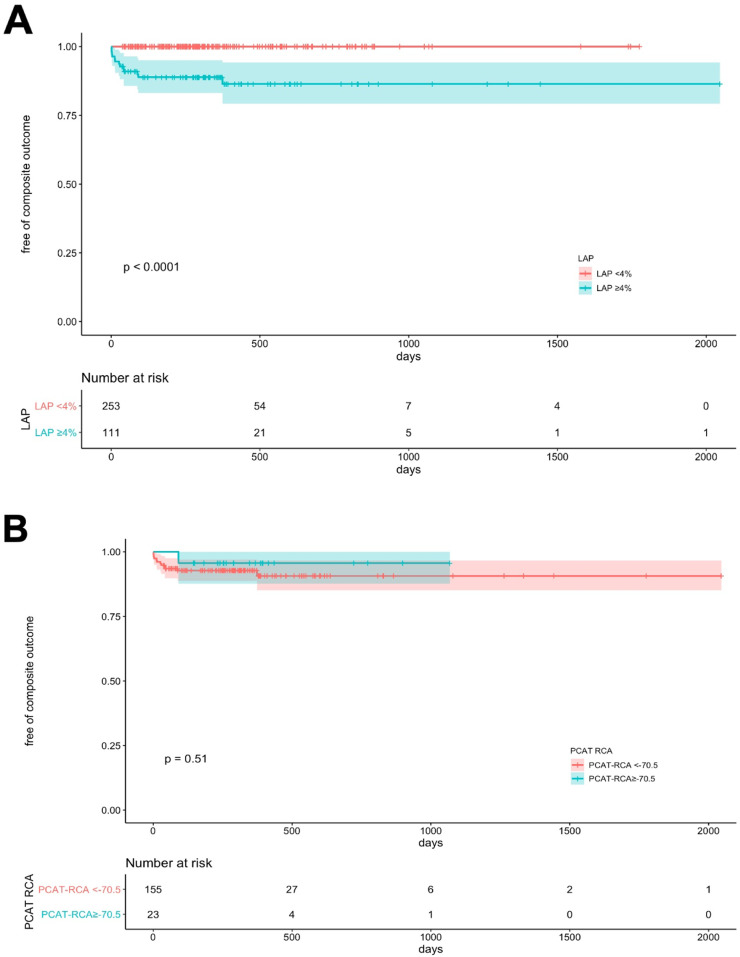
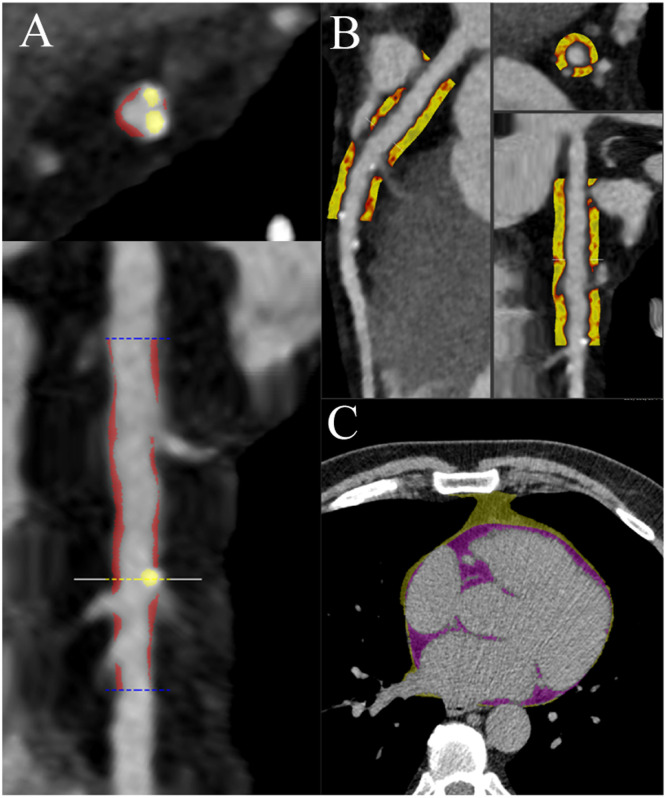
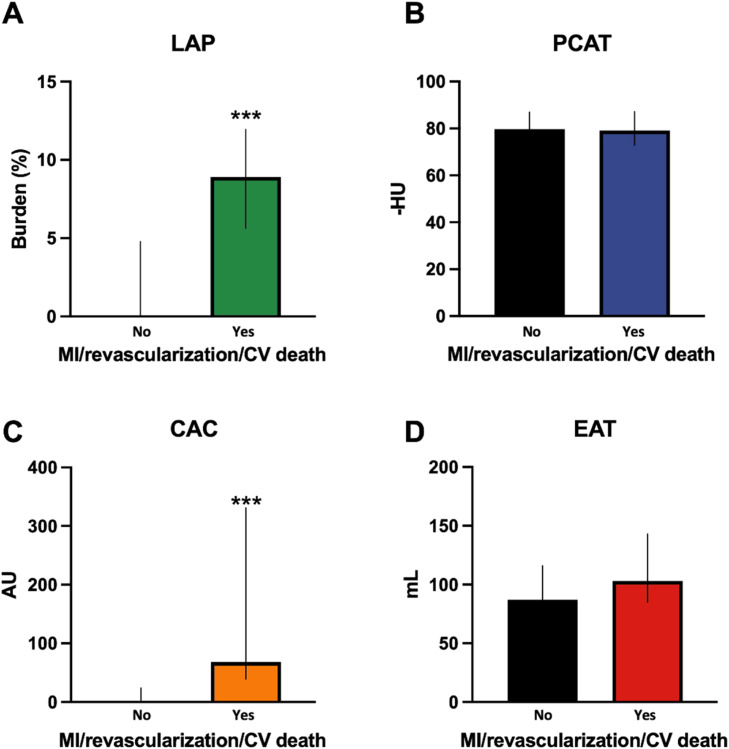
The patient population consisted of consecutive patients who underwent CCTA for stable chest pain and had a complete cardiometabolic panel including lipoprotein(a). Plaque, PCAT and EAT were measured from CT using semiautomated software. Elevated LAP burden and PCAT attenuation were defined as ≥4% and ≥70.5 HU, respectively. The primary clinical end-point was a composite of myocardial infarction, revascularization or cardiovascular death.
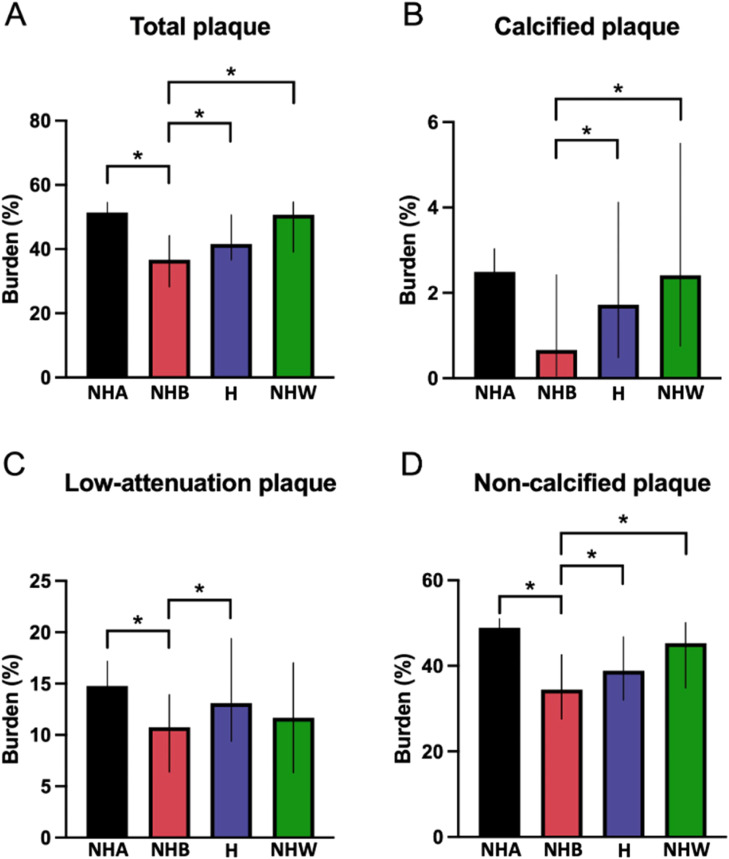
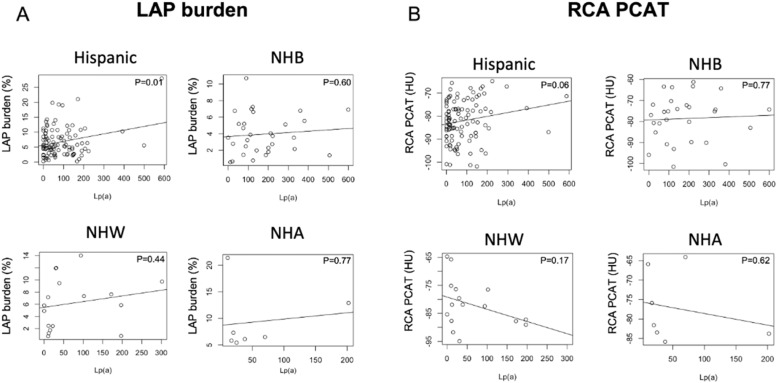
A total of 364 consecutive patients were included (median age 56 years, 64% female); the majority of patients were of Hispanic (60%), and the rest were of non-Hispanic Black (21%), non-Hispanic White (6%) and non-Hispanic Asian (4%) race/ethnicity. The prevalence of elevated LAP burden and PCAT attenuation was 31 and 18%, respectively, while only 8% had obstructive stenosis. There were significant differences in plaque characteristics among different racial/ethnic groups (p<0.001). Lipoprotein(a) correlated with LAP burden in Hispanic patients. Patients with elevated LAP were older, more likely to be have diabetes, hypertension, hyperlipidemia and smoke with higher CAC and EAT volume (all P<0.05). Patients with elevated LAP were more likely to develop the primary clinical outcome (p<0.001) but those with elevated PCAT were not (p=0.797).
The prevalence of LAP and PCAT attenuation were 31 and 18%, respectively. Lipoprotein(a) levels correlated with LAP burden in Hispanic patients. Age, male sex, hypertension and hyperlipidemia increased the odds of elevated LAP, which showed prognostic significance.
冠状动脉CT血管造影(CCTA)测量的低衰减非钙化斑块(LAP)负荷和冠状动脉周围脂肪组织(PCAT)引起的血管炎症已被证明是心血管结局的预测指标。我们旨在研究包括脂蛋白(a)和心外膜脂肪组织(EAT)在内的心脏代谢危险因素与CCTA高危成像生物标志物、LAP和血管炎症之间的关系。
患者群体包括因稳定型胸痛接受CCTA检查且有完整心脏代谢指标(包括脂蛋白(a))的连续患者。使用半自动软件从CT测量斑块、PCAT和EAT。LAP负荷升高和PCAT衰减分别定义为≥4%和≥70.5 HU。主要临床终点是心肌梗死、血运重建或心血管死亡的复合终点。
共纳入364例连续患者(中位年龄56岁,64%为女性);大多数患者为西班牙裔(60%),其余为非西班牙裔黑人(21%)、非西班牙裔白人(6%)和非西班牙裔亚洲人(4%)种族/族裔。LAP负荷升高和PCAT衰减的患病率分别为31%和18%,而只有8%有阻塞性狭窄。不同种族/族裔群体的斑块特征存在显著差异(p<0.001)。在西班牙裔患者中,脂蛋白(a)与LAP负荷相关。LAP升高的患者年龄更大,更有可能患有糖尿病、高血压、高脂血症且吸烟,冠状动脉钙化(CAC)和EAT体积更高(所有P<0.05)。LAP升高的患者更有可能发生主要临床结局(p<0.001),但PCAT升高的患者则不然(p=0.797)。
LAP和PCAT衰减的患病率分别为31%和18%。在西班牙裔患者中,脂蛋白(a)水平与LAP负荷相关。年龄、男性、高血压和高脂血症增加了LAP升高的几率,这具有预后意义。