Department of Liver Surgery, Sun Yat-sen University Cancer Center, 651 Dongfeng East Road, Guangzhou, China.
State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, 651 Dongfeng East Road, Guangzhou, China.
Eur J Med Res. 2023 Sep 9;28(1):328. doi: 10.1186/s40001-023-01310-4.
Lack of opportunity for radical surgery and postoperative tumor recurrence are challenges for surgeons and hepatocellular carcinoma (HCC) patients. This study aimed to develop nomograms to predict recurrence risk and recurrence-free survival (RFS) probability after conversion hepatectomy for patients previously receiving transarterial interventional therapy.
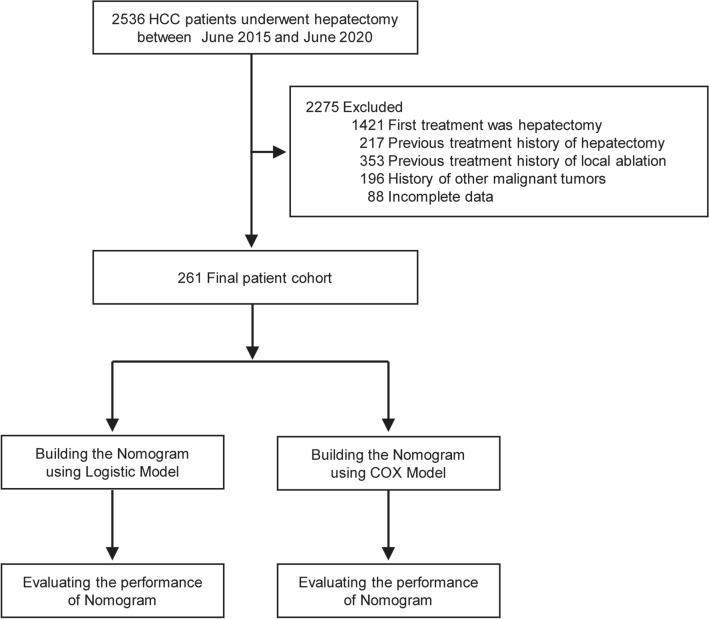
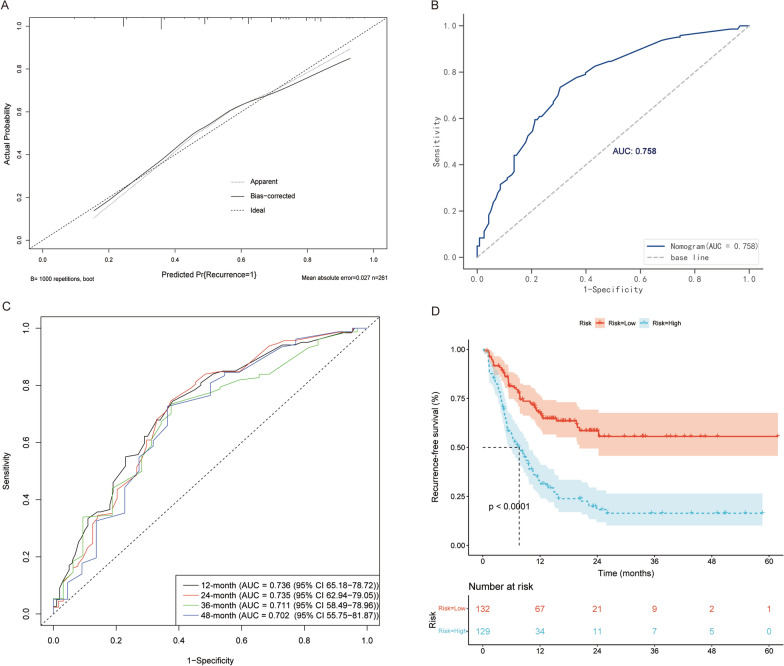
In total, 261 HCC patients who underwent conversion liver resection and previously received transarterial interventional therapy were retrospectively enrolled. Nomograms to predict recurrence risk and RFS were developed, with discriminative ability and calibration evaluated by C-statistics, calibration plots, and the Area under the Receiver Operator Characteristic (AUROC) curves.
Univariate/multivariable logistic regression and Cox regression analyses were used to identify predictive factors for recurrence risk and RFS, respectively. The following factors were selected as predictive of recurrence: age, tumor number, microvascular invasion (MVI) grade, preoperative alpha-fetoprotein (AFP), preoperative carbohydrate antigen 19-9 (CA19-9), and Eastern Cooperative Oncology Group performance score (ECOG PS). Similarly, age, tumor number, postoperative AFP, postoperative protein induced by vitamin K absence or antagonist-II (PIVKA-II), and ECOG PS were incorporated for the prediction of RFS. The discriminative ability and calibration of the nomograms revealed good predictive ability. Calibration plots showed good agreement between the nomogram predictions of recurrence and RFS and the actual observations.
A pair of reliable nomograms was developed to predict recurrence and RFS in HCC patients after conversion resection who previously received transarterial interventional therapy. These predictive models can be used as guidance for clinicians to help with treatment strategies.
根治性手术机会的缺乏和术后肿瘤复发是外科医生和肝细胞癌(HCC)患者面临的挑战。本研究旨在为先前接受经动脉介入治疗的患者开发用于预测转化肝切除术后复发风险和无复发生存(RFS)概率的列线图。
共回顾性纳入 261 例先前接受经动脉介入治疗后接受转化肝切除术的 HCC 患者。开发了用于预测复发风险和 RFS 的列线图,通过 C 统计量、校准图和接收者操作特征(ROC)曲线下面积(AUROC)曲线评估区分能力和校准。
单因素/多因素逻辑回归和 Cox 回归分析分别用于确定复发风险和 RFS 的预测因素。选择以下因素作为复发的预测因素:年龄、肿瘤数量、微血管侵犯(MVI)分级、术前甲胎蛋白(AFP)、术前碳水化合物抗原 19-9(CA19-9)和东部肿瘤协作组表现评分(ECOG PS)。同样,年龄、肿瘤数量、术后 AFP、术后维生素 K 缺乏或拮抗剂-II 诱导蛋白(PIVKA-II)和 ECOG PS 被纳入 RFS 的预测中。列线图的区分能力和校准显示出良好的预测能力。校准图显示列线图预测的复发和 RFS 与实际观察结果之间具有良好的一致性。
为先前接受经动脉介入治疗的转化切除术后 HCC 患者开发了一对可靠的列线图,用于预测复发和 RFS。这些预测模型可以作为临床医生的指导,帮助制定治疗策略。