Chylińska Magdalena, Komendziński Jakub, Wyszomirski Adam, Karaszewski Bartosz
Department of Adult Neurology, Gdańsk Medical University, Gdańsk, Poland.
Mult Scler Int. 2023 Aug 31;2023:4130557. doi: 10.1155/2023/4130557. eCollection 2023.
Currently, clinical trials of DMTs strive to determine their effect on neuroinflammation and neurodegeneration. We aimed to determine the impact of currently used DMTs on brain atrophy and disability in RRMS. The main goal of this review is to evaluate the neuroprotective potential of MS therapy and assess its impact on disability.
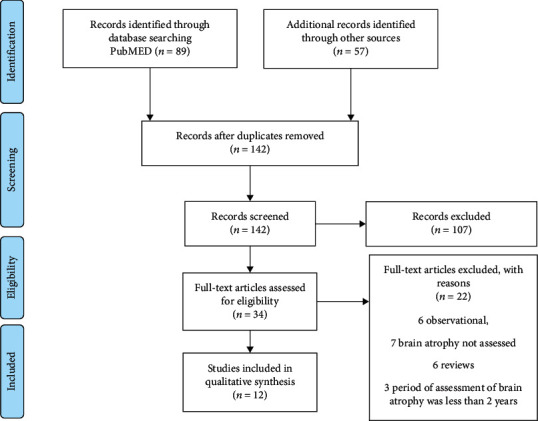
We performed a systematic analysis of clinical trials that used brain atrophy as an outcome or performed post hoc analysis of volumetric MRI parameters to assess the neuroprotective potential of applied therapies. Trials between 2008 and 2019 that included published results of brain parenchymal fraction (BPF) change and brain volume loss (BVL) in the period from baseline to week 96 or longer were considered.
Twelve from 146 clinical trials met the inclusion criteria and were incorporated into the analysis. DMTs that presented a large reduction in BVL also exhibited robust effects on clinical disability worsening, e.g., alemtuzumab with a 42% risk reduction in 6-month confirmed disability accumulation ( = 0.0084), ocrelizumab with a 40% risk reduction in 6-month confirmed disability progression ( = 0.003), and other DMTs (cladribine and teriflunomide) with moderate influence on brain atrophy were also associated with a marked impact on disability worsening. Dimethyl fumarate (DEFINE) and fingolimod (FREEDOMS I) initially exhibited significant effect on BVL; however, this effect was not confirmed in further clinical trials: CONFIRM and FREEDOMS II, respectively. Peg-IFN-1a shows a modest effect on BVL and disability worsening.
Our results show that BVL in one of the components of clinical disability worsening, together with other variables (lesion volume and annualized relapse rate). Standardization of atrophy measurement technique as well as harmonization of disability worsening and progression criteria in further clinical trials are of utmost importance as they enable a reliable comparison of neuroprotective potential of DMTs.
目前,疾病修正治疗药物(DMTs)的临床试验致力于确定其对神经炎症和神经退行性变的影响。我们旨在确定当前使用的DMTs对复发缓解型多发性硬化症(RRMS)患者脑萎缩和残疾的影响。本综述的主要目的是评估MS治疗的神经保护潜力并评估其对残疾的影响。
我们对以脑萎缩为结局的临床试验进行了系统分析,或对容积磁共振成像(MRI)参数进行事后分析,以评估所用治疗方法的神经保护潜力。纳入了2008年至2019年间的试验,这些试验包括从基线到第96周或更长时间的脑实质分数(BPF)变化和脑容量损失(BVL)的已发表结果。
146项临床试验中有12项符合纳入标准并纳入分析。BVL大幅降低的DMTs对临床残疾恶化也有显著影响,例如,阿仑单抗使6个月确诊残疾累积风险降低42%(P = 0.0084),奥瑞珠单抗使6个月确诊残疾进展风险降低40%(P = 0.003),其他对脑萎缩有中度影响的DMTs(克拉屈滨和特立氟胺)也与残疾恶化的显著影响相关。富马酸二甲酯(DEFINE)和芬戈莫德(FREEDOMS I)最初对BVL有显著影响;然而,在后续临床试验CONFIRM和FREEDOMS II中,这种效果未得到证实。聚乙二醇干扰素-1a对BVL和残疾恶化有适度影响。
我们的结果表明,BVL是临床残疾恶化的组成部分之一,与其他变量(病灶体积和年化复发率)一起。萎缩测量技术的标准化以及在进一步临床试验中残疾恶化和进展标准的统一至关重要,因为它们能够可靠地比较DMTs的神经保护潜力。