Department of Internal Medicine, Academic Center for Thyroid Diseases, Erasmus University Medical Center, Rotterdam, Netherlands; Department of Epidemiology, Erasmus University Medical Center, Rotterdam, Netherlands.
Department of Internal Medicine, Academic Center for Thyroid Diseases, Erasmus University Medical Center, Rotterdam, Netherlands.
Lancet Diabetes Endocrinol. 2023 Oct;11(10):743-754. doi: 10.1016/S2213-8587(23)00227-9. Epub 2023 Sep 8.
Reference intervals of thyroid-stimulating hormone (TSH) and free thyroxine (FT) are statistically defined by the 2·5-97·5th percentiles, without accounting for potential risk of clinical outcomes. We aimed to define the optimal healthy ranges of TSH and FT based on the risk of cardiovascular disease and mortality.
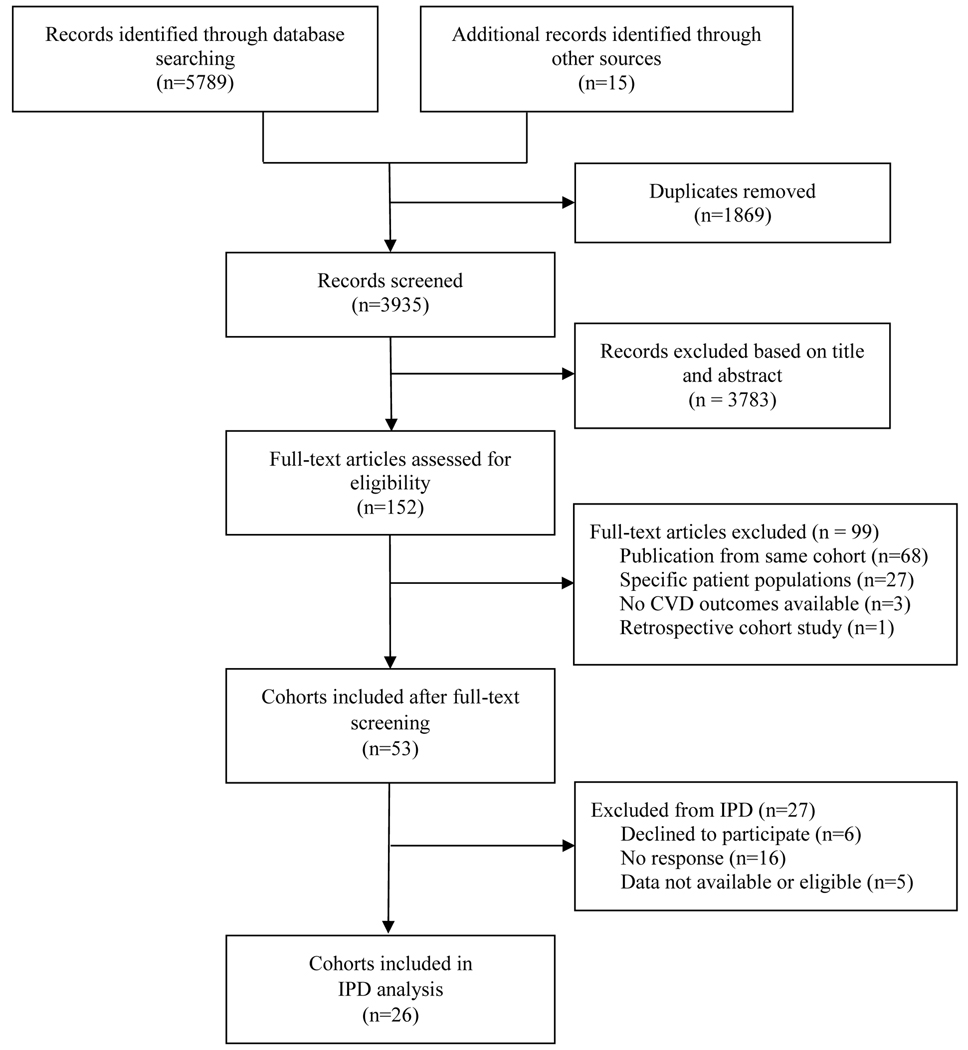
This systematic review and individual participant data (IPD) meta-analysis identified eligible prospective cohorts through the Thyroid Studies Collaboration, supplemented with a systematic search via Embase, MEDLINE (Ovid), Web of science, the Cochrane Central Register of Controlled Trials, and Google Scholar from Jan 1, 2011, to Feb 12, 2017 with an updated search to Oct 13, 2022 (cohorts found in the second search were not included in the IPD). We included cohorts that collected TSH or FT, and cardiovascular outcomes or mortality for adults (aged ≥18 years). We excluded cohorts that included solely pregnant women, individuals with overt thyroid diseases, and individuals with cardiovascular disease. We contacted the study investigators of eligible cohorts to provide IPD on demographics, TSH, FT, thyroid peroxidase antibodies, history of cardiovascular disease and risk factors, medication use, cardiovascular disease events, cardiovascular disease mortality, and all-cause mortality. The primary outcome was a composite outcome including cardiovascular disease events (coronary heart disease, stroke, and heart failure) and all-cause mortality. Secondary outcomes were the separate assessment of cardiovascular disease events, all-cause mortality, and cardiovascular disease mortality. We performed one-step (cohort-stratified Cox models) and two-step (random-effects models) meta-analyses adjusting for age, sex, smoking, systolic blood pressure, diabetes, and total cholesterol. The study was registered with PROSPERO, CRD42017057576.
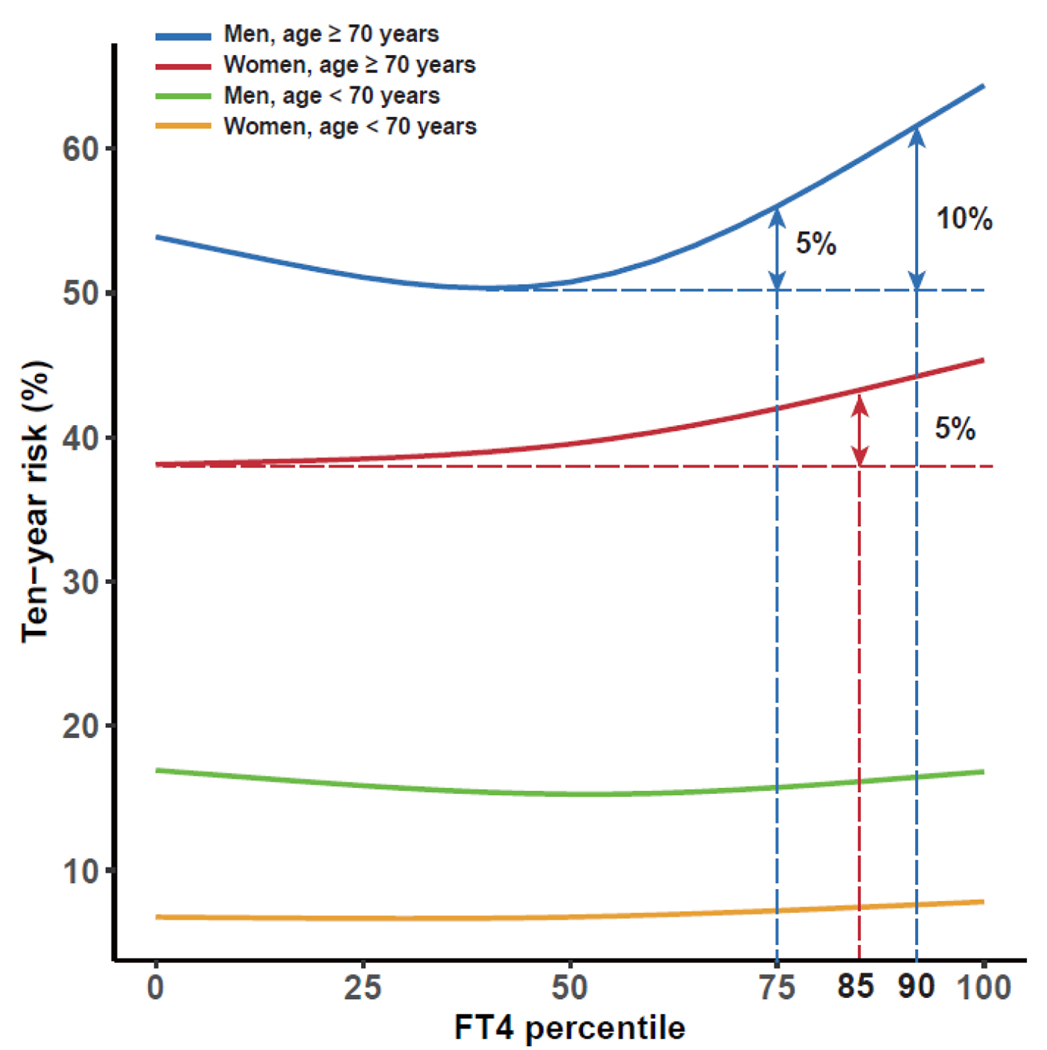
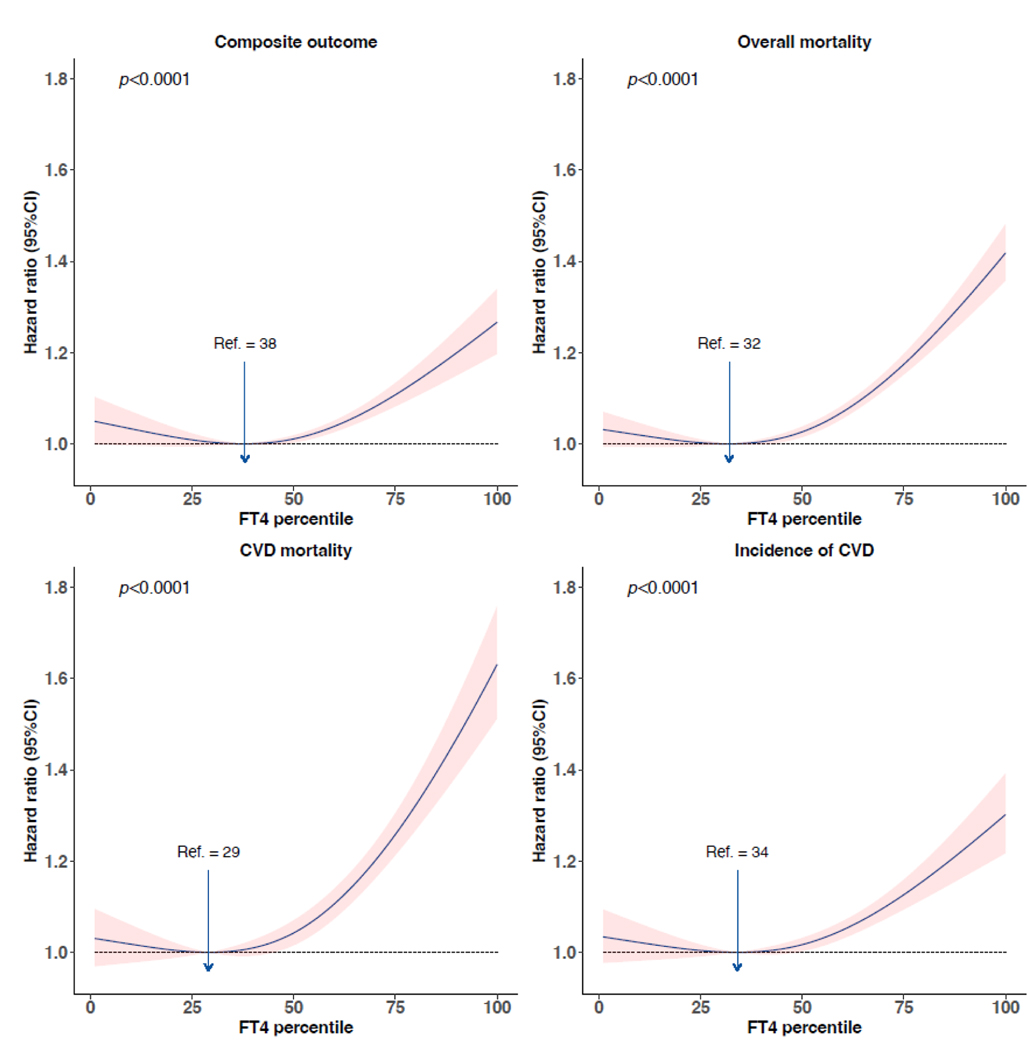
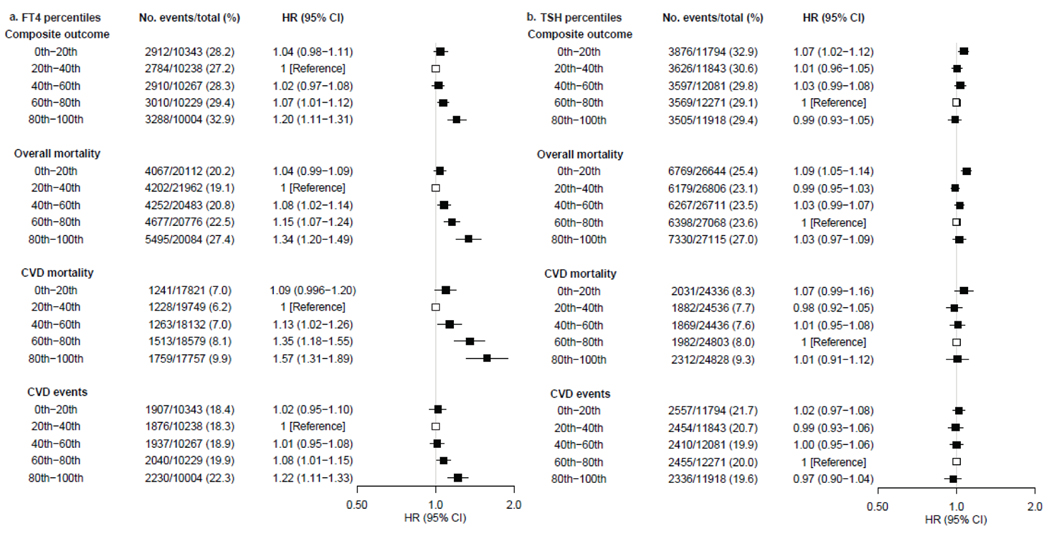
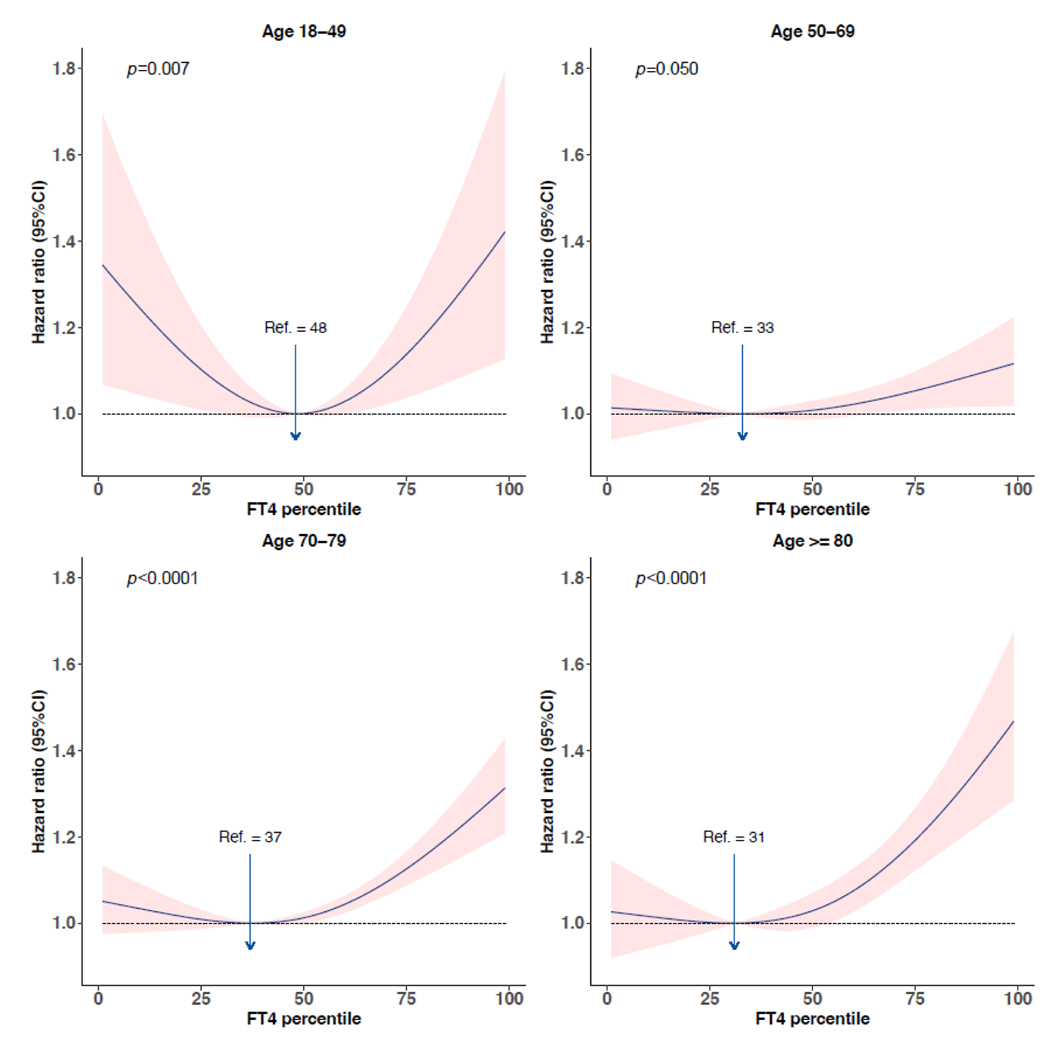
We identified 3935 studies, of which 53 cohorts fulfilled the inclusion criteria and 26 cohorts agreed to participate. We included IPD on 134 346 participants with a median age of 59 years (range 18-106) at baseline. There was a J-shaped association of FT with the composite outcome and secondary outcomes, with the 20th (median 13·5 pmol/L [IQR 11·2-13·9]) to 40th percentiles (median 14·8 pmol/L [12·3-15·0]) conveying the lowest risk. Compared with the 20-40th percentiles, the age-adjusted and sex-adjusted hazard ratio (HR) for FT in the 80-100th percentiles was 1·20 (95% CI 1·11-1·31) for the composite outcome, 1·34 (1·20-1·49) for all-cause mortality, 1·57 (1·31-1·89) for cardiovascular disease mortality, and 1·22 (1·11-1·33) for cardiovascular disease events. In individuals aged 70 years and older, the 10-year absolute risk of composite outcome increased over 5% for women with FT greater than the 85th percentile (median 17·6 pmol/L [IQR 15·0-18·3]), and men with FT greater than the 75th percentile (16·7 pmol/L [14·0-17·4]). Non-linear associations were identified for TSH, with the 60th (median 1·90 mIU/L [IQR 1·68-2·25]) to 80th percentiles (2·90 mIU/L [2·41-3·32]) associated with the lowest risk of cardiovascular disease and mortality. Compared with the 60-80th percentiles, the age-adjusted and sex-adjusted HR of TSH in the 0-20th percentiles was 1·07 (95% CI 1·02-1·12) for the composite outcome, 1·09 (1·05-1·14) for all-cause mortality, and 1·07 (0·99-1·16) for cardiovascular disease mortality.
There was a J-shaped association of FT with cardiovascular disease and mortality. Low concentrations of TSH were associated with a higher risk of all-cause mortality and cardiovascular disease mortality. The 20-40th percentiles of FT and the 60-80th percentiles of TSH could represent the optimal healthy ranges of thyroid function based on the risk of cardiovascular disease and mortality, with more than 5% increase of 10-year composite risk identified for FT greater than the 85th percentile in women and men older than 70 years. We propose a feasible approach to establish the optimal healthy ranges of thyroid function, allowing for better identification of individuals with a higher risk of thyroid-related outcomes.
None.
促甲状腺激素(TSH)和游离甲状腺素(FT)的参考区间是通过第 2.5-97.5 百分位数进行统计学定义的,没有考虑到潜在的临床结局风险。我们旨在根据心血管疾病和死亡率的风险,定义 TSH 和 FT 的最佳健康范围。
本系统评价和个体参与者数据(IPD)荟萃分析通过甲状腺研究协作组织确定了合格的前瞻性队列,并通过 Embase、MEDLINE(Ovid)、Web of Science、Cochrane 对照试验中心注册库和 Google Scholar 进行了系统搜索,搜索时间从 2011 年 1 月 1 日至 2017 年 2 月 12 日,更新搜索时间为 2022 年 10 月 13 日(第二次搜索中发现的队列不包括在 IPD 中)。我们纳入了收集 TSH 或 FT 以及心血管结局或成年人死亡率的队列。我们排除了仅包含孕妇、患有显性甲状腺疾病和患有心血管疾病的队列。我们联系了合格队列的研究调查人员,以提供关于人口统计学、TSH、FT、甲状腺过氧化物酶抗体、心血管疾病和危险因素史、药物使用、心血管疾病事件、心血管疾病死亡率和全因死亡率的 IPD。主要结局是包括心血管疾病事件(冠心病、中风和心力衰竭)和全因死亡率的复合结局。次要结局是对心血管疾病事件、全因死亡率和心血管疾病死亡率的单独评估。我们进行了一步(队列分层 Cox 模型)和两步(随机效应模型)荟萃分析,调整了年龄、性别、吸烟、收缩压、糖尿病和总胆固醇。该研究已在 PROSPERO 注册,CRD42017057576。
我们确定了 3935 项研究,其中 53 项队列符合纳入标准,26 项队列同意参与。我们纳入了 134346 名参与者的 IPD,中位年龄为 59 岁(范围 18-106 岁)。FT 与复合结局和次要结局呈 J 形关联,第 20(中位数 13.5 pmol/L [11.2-13.9])至 40(中位数 14.8 pmol/L [12.3-15.0])百分位传递出最低的风险。与第 20-40 百分位相比,第 80-100 百分位的 FT 的年龄调整和性别调整的危险比(HR)为复合结局 1.20(95%CI 1.11-1.31),全因死亡率 1.34(1.20-1.49),心血管疾病死亡率 1.57(1.31-1.89),心血管疾病事件 1.22(1.11-1.33)。在 70 岁及以上的人群中,女性 FT 大于第 85 百分位(中位数 17.6 pmol/L [15.0-18.3])和男性 FT 大于第 75 百分位(16.7 pmol/L [14.0-17.4])的 10 年复合结局绝对风险增加超过 5%。TSH 存在非线性关联,第 60(中位数 1.90 mIU/L [1.68-2.25])至 80(中位数 2.90 mIU/L [2.41-3.32])百分位与心血管疾病和死亡率的最低风险相关。与第 60-80 百分位相比,第 0-20 百分位的 TSH 的年龄调整和性别调整的 HR 为复合结局 1.07(95%CI 1.02-1.12),全因死亡率 1.09(1.05-1.14),心血管疾病死亡率 1.07(0.99-1.16)。
FT 与心血管疾病和死亡率呈 J 形关联。低浓度的 TSH 与全因死亡率和心血管疾病死亡率的风险增加相关。FT 的第 20-40 百分位和 TSH 的第 60-80 百分位可能代表基于心血管疾病和死亡率风险的甲状腺功能的最佳健康范围,女性大于 70 岁和男性大于 70 岁的 FT 大于第 85 百分位的人群中,10 年复合风险增加超过 5%。我们提出了一种可行的方法来确定甲状腺功能的最佳健康范围,从而更好地识别与甲状腺相关结局风险较高的个体。
无。