Bureau de Biostatistique et d'Epidémiologie, Gustave Roussy, Université Paris-Saclay, Villejuif, France.
Oncostat U1018, Inserm, Université Paris-Saclay, Equipe labellisée Ligue Contre le Cancer, 114 Rue Edouard Vaillant, Villejuif, France.
Br J Cancer. 2023 Oct;129(9):1516-1523. doi: 10.1038/s41416-023-02420-w. Epub 2023 Sep 11.
Several randomized clinical trials provide evidence of the survival benefit of extended adjuvant tamoxifen in women with estrogen receptor (ER)-positive early breast cancer (BC). However, non-adherence may lead to underestimate treatment effects using intention to treat (ITT) methods. We reanalyzed a randomized trial using contemporary statistical methods adjusting for non-adherence.
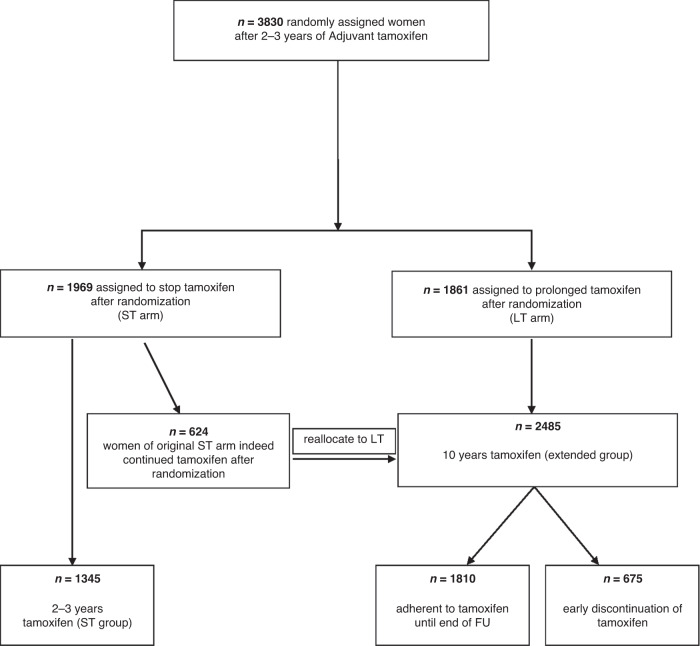
The TAM01 study was a phase 3 trial including women with early BC, who had completed 2-3 years of adjuvant tamoxifen between 1986 and 1995. Participants were randomly assigned to continue tamoxifen up to 10 years or to discontinue the treatment at randomization. Invasive disease-free survival (iDFS) and overall survival (OS) were estimated using marginal structural models (MSM) and rank preserving structural failure time model (RPSFTM).
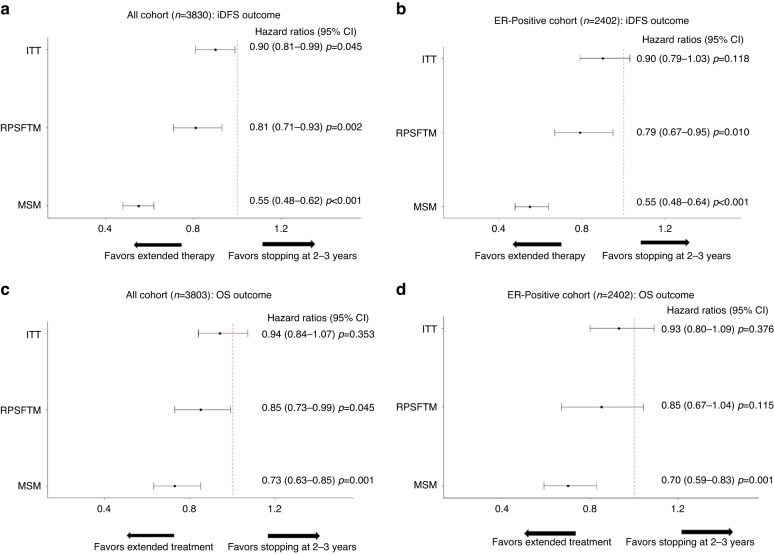
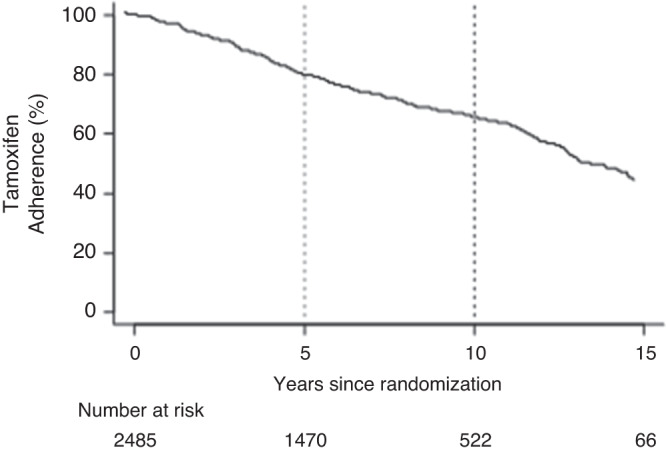
Of 3830 patients enrolled, 2485 were randomized to extended tamoxifen, and 1345 to treatment discontinuation. The 10-year non-adherence rate in the extended group was 27.2%. Among women with ER-positive BC (n = 2402), extended tamoxifen was associated with a 45% and 21% relative improvement in iDFS by MSM and RPSFTM, respectively (Hazard Ratio (HR), 0.55; 95% Confidence Interval (CI), 0.48-0.64 and HR, 0.79; 95%CI, 0.67-0.95, respectively), a considerable greater benefit than in the ITT analysis (HR, 0.90; 95%CI, 0.81-0.99). The OS reanalysis revealed a substantial benefit of extended tamoxifen (MSM: HR, 0.70; 95%CI, 0.59-0.83; RPSFTM: HR, 0.85; 95%CI, 0.67-1.04), compared to the ITT analyses (HR, 0.94; 95%CI, 0.84-1.07).
This analysis emphasizes both the importance of adherence to hormonotherapy in hormone-receptor positive early BC and the usefulness of more complex statistical analyses.
几项随机临床试验提供了证据,表明延长辅助他莫昔芬治疗雌激素受体(ER)阳性早期乳腺癌(BC)可延长患者的生存时间。然而,采用意向治疗(ITT)方法可能会低估不依从治疗的影响。我们使用当代统计学方法,对一项随机试验进行了再分析,对不依从治疗进行了调整。
TAM01 研究是一项 3 期临床试验,纳入了 1986 年至 1995 年期间完成 2-3 年辅助他莫昔芬治疗的早期 BC 女性患者。参与者被随机分配继续接受他莫昔芬治疗至 10 年或在随机分组时停止治疗。使用边缘结构模型(MSM)和秩保留结构失效时间模型(RPSFTM)估计无侵袭性疾病生存(iDFS)和总生存(OS)。
在纳入的 3830 例患者中,2485 例被随机分配至延长组接受他莫昔芬治疗,1345 例被随机分配至停止治疗组。延长组的 10 年不依从率为 27.2%。在 ER 阳性 BC 患者中(n=2402),MSM 和 RPSFTM 分别显示延长组 iDFS 相对改善 45%和 21%(风险比(HR),0.55;95%置信区间(CI),0.48-0.64 和 HR,0.79;95%CI,0.67-0.95),这表明与 ITT 分析相比,获益更大(HR,0.90;95%CI,0.81-0.99)。OS 的再分析显示,与 ITT 分析相比,延长他莫昔芬治疗有显著获益(MSM:HR,0.70;95%CI,0.59-0.83;RPSFTM:HR,0.85;95%CI,0.67-1.04)。
本分析强调了在激素受体阳性早期 BC 中坚持激素治疗的重要性,以及更复杂的统计分析的有用性。