Division of Pulmonary and Critical Care.
Center for Global Non-Communicable Disease Research and Training, School of Medicine, and.
Am J Respir Crit Care Med. 2023 Nov 15;208(10):1052-1062. doi: 10.1164/rccm.202303-0505OC.
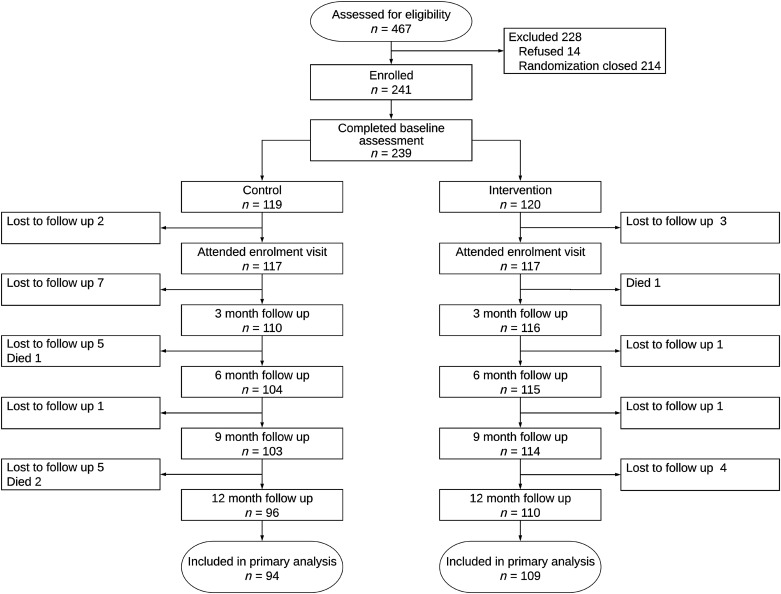
Chronic obstructive pulmonary disease (COPD) disproportionately affects low- and middle-income countries. Health systems are ill prepared to manage the increase in COPD cases. We performed a pilot effectiveness-implementation randomized field trial of a community health worker (CHW)-supported, 1-year self-management intervention in individuals with COPD grades B-D. The study took place in low-resource settings of Nepal, Peru, and Uganda. The primary outcome was the St. George's Respiratory Questionnaire (SGRQ) score at 1 year. We evaluated differences in moderate to severe exacerbations, all-cause hospitalizations, and the EuroQol score (EQ-5D-3 L) at 12 months. We randomly assigned 239 participants (119 control arm, 120 intervention arm) with grades B-D COPD to a multicomponent, CHW-supported intervention or standard of care and COPD education. Twenty-five participants (21%) died or were lost to follow-up in the control arm compared with 11 (9%) in the intervention arm. At 12 months, there was no difference in mean total SGRQ score between the intervention and control arms (34.7 vs. 34.0 points; adjusted mean difference, 1.0; 95% confidence interval, -4.2, 6.1; = 0.71). The intervention arm had a higher proportion of hospitalizations than the control arm (10% vs. 5.2%; adjusted odds ratio, 2.2; 95% confidence interval, 0.8, 7.5; = 0.15) at 12 months. A CHW-based intervention to support self-management of acute exacerbations of COPD in three resource-poor settings did not result in differences in SGRQ scores at 1 year. Fidelity was high, and intervention engagement was moderate. Although these results cannot differentiate between a failed intervention or implementation, they nonetheless suggest that we need to revisit our strategy. Clinical trial registered with www.clinicaltrials.gov (NCT03359915).
慢性阻塞性肺疾病(COPD)在中低收入国家的发病率较高。卫生系统尚未准备好应对 COPD 病例的增加。我们在尼泊尔、秘鲁和乌干达的资源匮乏地区开展了一项关于社区卫生工作者(CHW)支持的为期 1 年 COPD 患者自我管理干预的试点有效性-实施随机现场试验。主要结局指标为 1 年时的圣乔治呼吸问卷(SGRQ)评分。我们评估了 12 个月时中度至重度恶化、全因住院和 EQ-5D-3L 评分的差异。我们将 239 名 B-D 级 COPD 患者随机分为多组分、CHW 支持的干预组或对照组(标准护理和 COPD 教育)。对照组有 25 名(21%)参与者死亡或失访,而干预组有 11 名(9%)。12 个月时,干预组和对照组之间 SGRQ 总分平均差异无统计学意义(34.7 对 34.0 分;调整平均差异,1.0;95%置信区间,-4.2,6.1; = 0.71)。与对照组相比,干预组的住院率更高(10%对 5.2%;调整比值比,2.2;95%置信区间,0.8,7.5; = 0.15)。在三个资源匮乏的地区,基于 CHW 的干预措施来支持 COPD 急性加重的自我管理,并未导致 1 年后 SGRQ 评分的差异。一致性很高,干预参与率为中等。尽管这些结果无法区分干预失败或实施失败,但它们表明我们需要重新审视我们的策略。该临床试验已在 www.clinicaltrials.gov(NCT03359915)注册。