Yordanov Stefan, Yang Xiaoyu, Mowforth Oliver, K Demetriades Andreas, Ivanov Marcel, Vergara Pierluigi, Gardner Adrian, Pereira Erlick, Bateman Antony, Alamri Alexander, Francis Jibin, Trivedi Rikin, Kotter Mark, Davies Benjamin, Budu Alexandru
Academic Neurosurgery Unit, Department of Clinical Neurosurgery, Cambridge University, Cambridge, United Kingdom.
Department of Neurosurgery, Royal Infirmary Edinburgh, Edinburgh, United Kingdom.
JMIR Form Res. 2023 Sep 12;7:e48321. doi: 10.2196/48321.
Degenerative cervical myelopathy (DCM) is estimated to affect 2% of the adult population. DCM occurs when degenerative processes cause compression and injure the spinal cord. Surgery to remove the stress caused by the compression of the spinal cord is the mainstay of treatment, with a range of techniques in use. Although various factors are described to inform the selection of these techniques, there needs to be more consensus and limited comparative evidence.
The main objective of this survey was to explore the variation of practice and decision-making, with a focus on laminectomy versus laminectomy and fusion in posterior surgery of the cervical spine. We present the results of a survey conducted among the principal investigators (PIs) of the National Institute for Health and Care Research (NIHR) randomized controlled trial on posterior laminectomy with fixation for degenerative cervical myelopathy (POLYFIX-DCM).
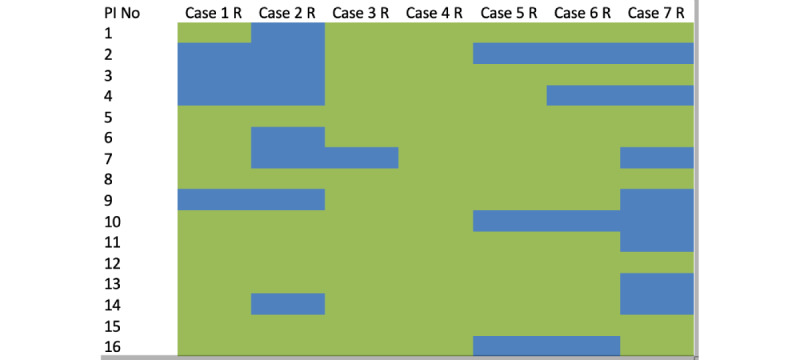
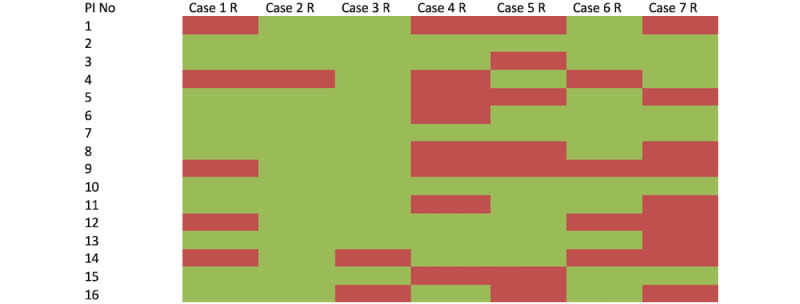
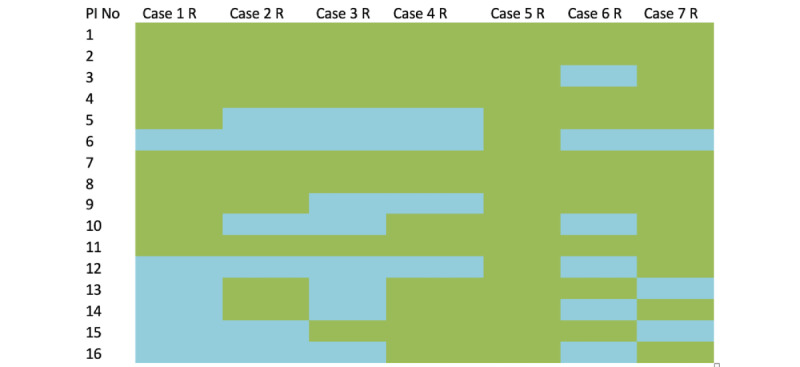
A series of 7 cases were shared with 24 PIs using SurveyMonkey. Each case consisted of a midsagittal T2-weighted magnetic resonance imaging and lateral cervical x-rays in flexion and extension. Surgeons were asked if their preferred approach was anterior or posterior. If posterior, they were asked whether they preferred to instrument and whether they had the equipoise to randomize in the NIHR POLYFIX-DCM trial. Variability in decision-making was then explored using factors reported to inform decision-making, such as alignment, location of compression, number of levels operated, presence of mobile spondylolisthesis, and patient age.
The majority of PIs (16/30, 53%) completed the survey. Overall, PIs favored a posterior approach (12/16, 75%) with instrumentation (75/112, average 66%) and would randomize (67/112, average 62%) most cases. Factors reported to inform decision-making poorly explained variability in responses in both univariate testing and with a multivariate model (R2=0.1). Only surgeon experience of more than 5 years and orthopedic specialty training background were significant predictors, both associated with an anterior approach (odds ratio [OR] 1.255; P=.02 and OR 1.344; P=.007, respectively) and fusion for posterior procedures (OR 0.628; P<.001 and OR 1.344; P<.001, respectively). Surgeon experience also significantly affected the openness to randomize, with those with more than 5 years of experience less likely to randomize (OR -0.68; P<.001).
In this representative sample of spine surgeons participating in the POLYFIX-DCM trial as investigators, there is no consensus on surgical strategy, including the role of instrumented fusion following posterior decompression. Overall, this study supports the view that there appears to be a clinical equipoise, and conceptually, a randomized controlled trial appears feasible, which sets the scene for the NIHR POLYFIX-DCM trial.
据估计,退行性颈椎脊髓病(DCM)影响2%的成年人口。当退行性病变导致脊髓受压并受损时,就会发生DCM。通过手术消除脊髓受压所产生的压力是主要治疗手段,目前有多种技术可供使用。尽管有多种因素可用于指导这些技术的选择,但仍需要更多的共识以及有限的比较证据。
本次调查的主要目的是探讨手术实践和决策的差异,重点是颈椎后路手术中单纯椎板切除术与椎板切除融合术的比较。我们展示了一项针对英国国家健康与照护研究机构(NIHR)关于退行性颈椎脊髓病后路椎板切除内固定术(POLYFIX-DCM)随机对照试验的主要研究者(PI)所进行的调查结果。
使用SurveyMonkey向24位主要研究者分享了一系列7个病例。每个病例包括一张矢状面T2加权磁共振成像以及颈椎屈伸位的侧位X线片。询问外科医生他们首选的手术入路是前路还是后路。如果是后路,询问他们是否倾向于使用内固定器械,以及他们是否在NIHR的POLYFIX-DCM试验中有随机分组的平衡心态。然后利用报告的用于指导决策的因素,如对线情况、受压位置、手术节段数量、是否存在动态椎体滑脱以及患者年龄,来探讨决策的变异性。
大多数主要研究者(16/30,53%)完成了调查。总体而言,主要研究者更倾向于后路手术入路(12/16,75%)并使用内固定器械(75/112,平均66%),并且大多数病例愿意进行随机分组(67/112,平均62%)。在单变量测试和多变量模型中,报告的用于指导决策的因素都很难解释回答的变异性(R2 = 0.1)。只有超过5年的外科医生经验以及骨科专业培训背景是显著的预测因素,二者均与前路手术入路相关(优势比[OR]分别为1.255;P = 0.02和OR 1.344;P = 0.007),以及后路手术的融合相关(OR分别为0.628;P < 0.001和OR 1.344;P < 0.001)。外科医生经验也显著影响随机分组的意愿,经验超过5年的医生进行随机分组的可能性较小(OR -0.68;P < 0.001)。
在作为研究者参与POLYFIX-DCM试验的脊柱外科医生的这个代表性样本中,对于手术策略,包括后路减压后使用内固定融合的作用,没有达成共识。总体而言,本研究支持这样一种观点,即似乎存在临床平衡,从概念上讲,一项随机对照试验似乎是可行的,这为NIHR的POLYFIX-DCM试验奠定了基础。