Division of Hematology-Oncology, University of Alabama at Birmingham, Birmingham, AL.
Division of Hematology, Mayo Clinic, Rochester, MN.
Blood Adv. 2023 Nov 14;7(21):6568-6578. doi: 10.1182/bloodadvances.2023010706.
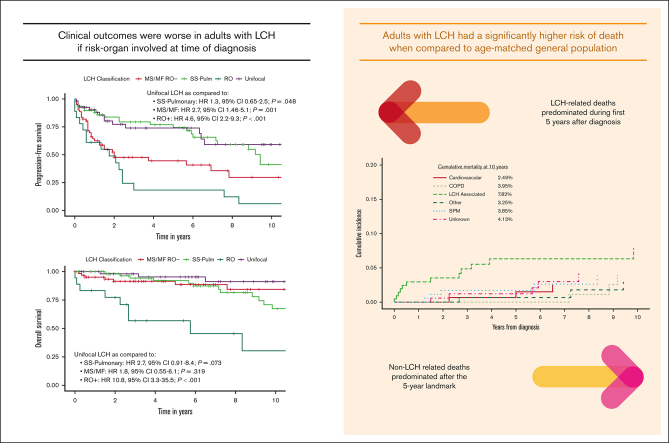
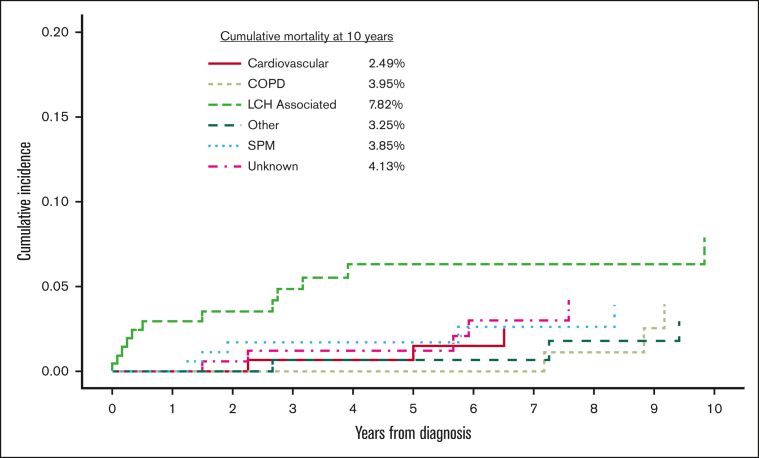
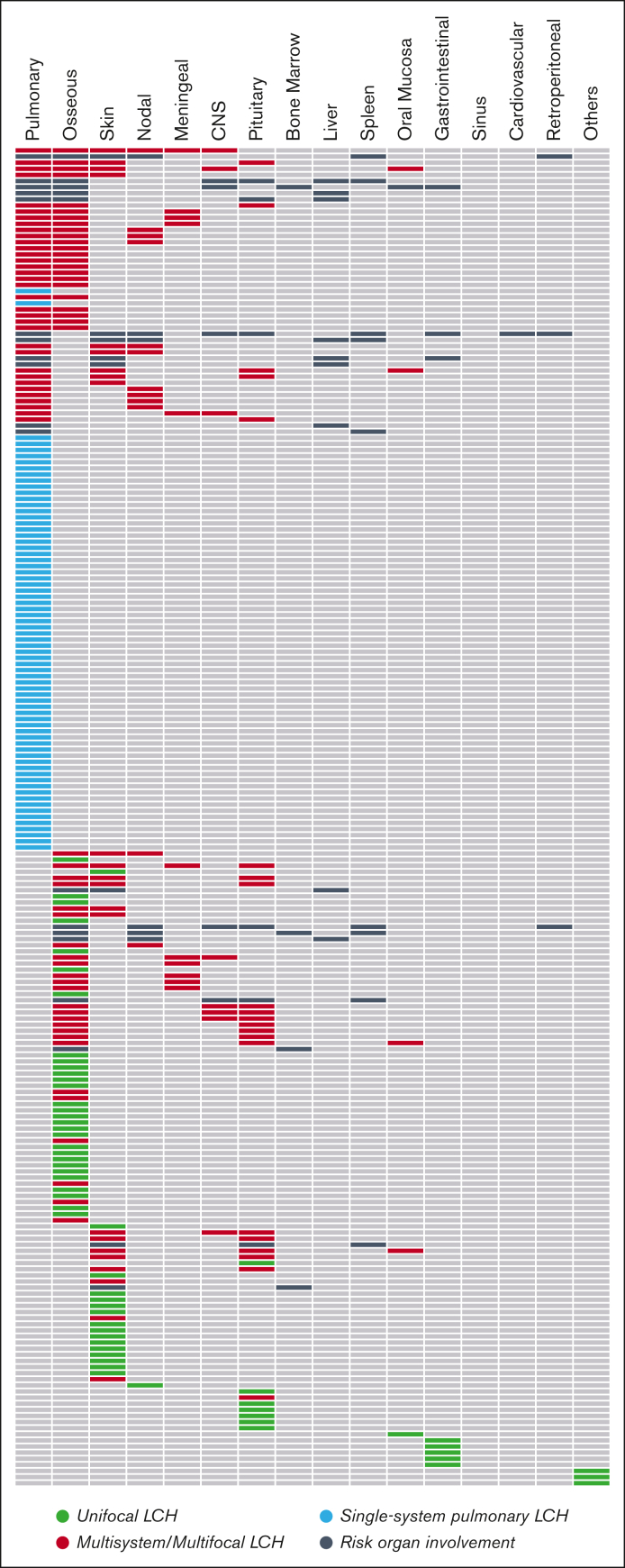
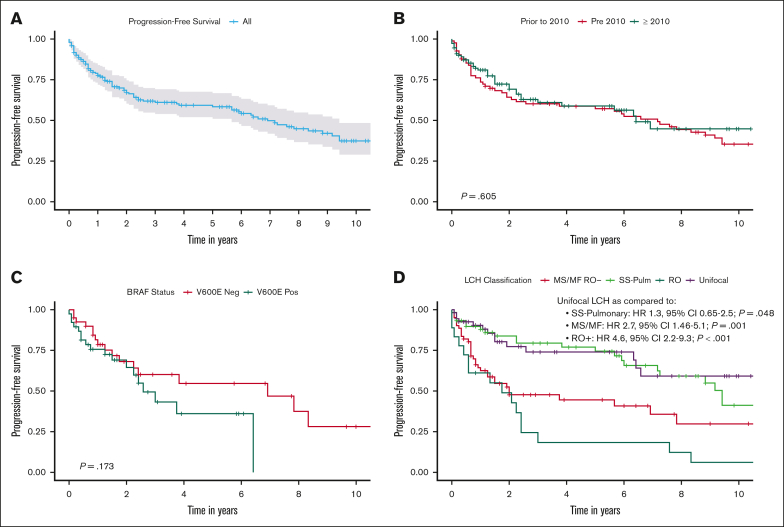
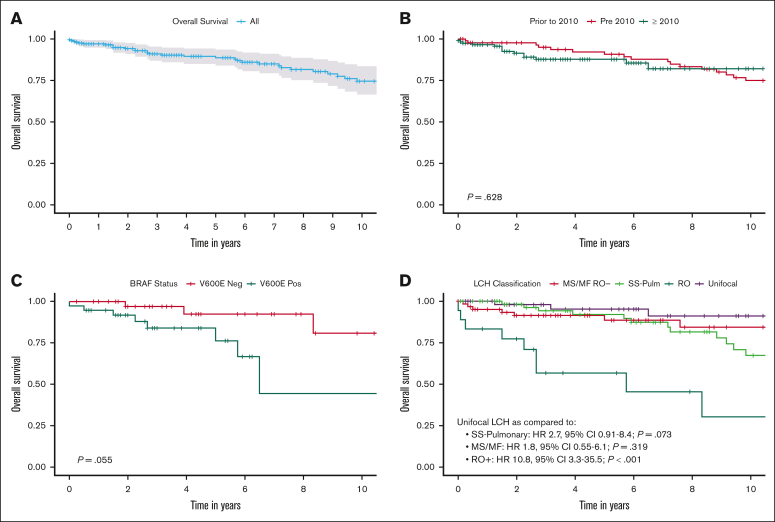
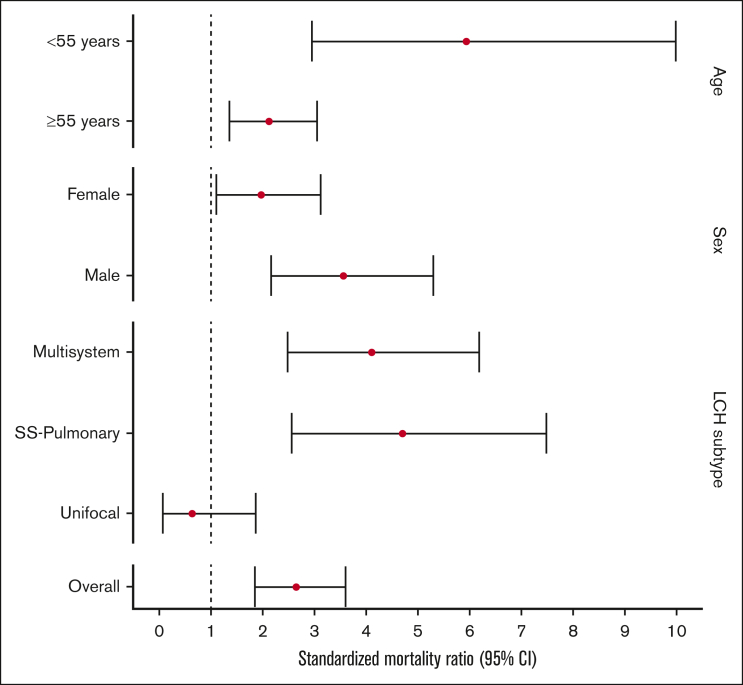
Advances in the treatment of Langerhans cell histiocytosis (LCH) have resulted in a growing survivor population. There is a lack of data on long-term outcomes among adults with LCH. We conducted a retrospective record review of 219 adults (aged ≥18 years) with LCH. Most common presentation was multisystem (34.2%), followed by single-system pulmonary (32%), unifocal (28.3%), and single-system multifocal (5.5%) LCH. Risk organ involvement (the liver, spleen, or bone marrow) was seen in 8.7% of cases, and 40 of 88 (45.5%) tested cases were BRAFV600E. At a median follow-up of 74 months, 5-year progression-free survival (PFS) was 58.3% and estimated median PFS was 83 months. Median overall survival (OS) was not reached; 5- and 10-year OS rates were 88.7% and 74.5%, respectively. Risk organ involvement was associated with worse PFS (hazard ratio [HR], 4.5) and OS (HR, 10.8). BRAFV600E was not associated with risk organ involvement or survival. When compared with matched unaffected US population, individuals with LCH had a significantly higher risk of overall mortality (standardized mortality ratio [SMR], 2.66), specifically among those aged <55 years at diagnosis (SMR, 5.94) and those with multisystem disease (SMR, 4.12). Second cancers occurred in 16.4% cases, including diverse hematologic and solid organ malignancies. LCH-associated deaths constituted 36.1% of deaths and occurred within 5 years of diagnosis. After 5 years, non-LCH causes of death, including second cancers, chronic obstructive pulmonary disease, and cardiovascular diseases, predominated. Our study highlights, to our knowledge, for the first time, that adults with LCH experience early and late mortality from non-LCH causes and the need for development of targeted survivorship programs to improve outcomes.
朗格汉斯细胞组织细胞增生症(LCH)的治疗进展导致生存者人数不断增加。目前缺乏成人 LCH 长期结果的数据。我们对 219 例成人(年龄≥18 岁)的 LCH 进行了回顾性病历审查。最常见的表现为多系统(34.2%),其次是单系统肺(32%)、单灶(28.3%)和单系统多灶(5.5%)LCH。风险器官受累(肝脏、脾脏或骨髓)见于 8.7%的病例,88 例检测病例中有 40 例(45.5%)为 BRAFV600E。中位随访 74 个月时,5 年无进展生存率(PFS)为 58.3%,估计中位 PFS 为 83 个月。中位总生存期(OS)未达到;5 年和 10 年 OS 率分别为 88.7%和 74.5%。风险器官受累与较差的 PFS(风险比[HR],4.5)和 OS(HR,10.8)相关。BRAFV600E 与风险器官受累或生存无关。与匹配的未受影响的美国人群相比,患有 LCH 的个体的总死亡率明显更高(标准化死亡率比[SMR],2.66),尤其是在诊断时年龄<55 岁的个体(SMR,5.94)和患有多系统疾病的个体(SMR,4.12)。16.4%的病例发生了第二癌症,包括各种血液系统和实体器官恶性肿瘤。LCH 相关死亡占死亡人数的 36.1%,发生在诊断后 5 年内。5 年后,非 LCH 导致的死亡,包括第二癌症、慢性阻塞性肺疾病和心血管疾病,占主导地位。我们的研究首次强调,据我们所知,成人 LCH 存在早期和晚期非 LCH 原因导致的死亡,需要制定针对性的生存方案以改善结果。