Ghosal Anit, Qadeer Hafiza Amna, Nekkanti Sravan K, Pradhan Priyanka, Okoye Chiugo, Waqar Danish
Internal Medicine, Kolkata Medical College and Hospital, Kolkata, IND.
Internal Medicine, Foundation University Medical College, Islamabad, PAK.
Cureus. 2023 Aug 12;15(8):e43390. doi: 10.7759/cureus.43390. eCollection 2023 Aug.
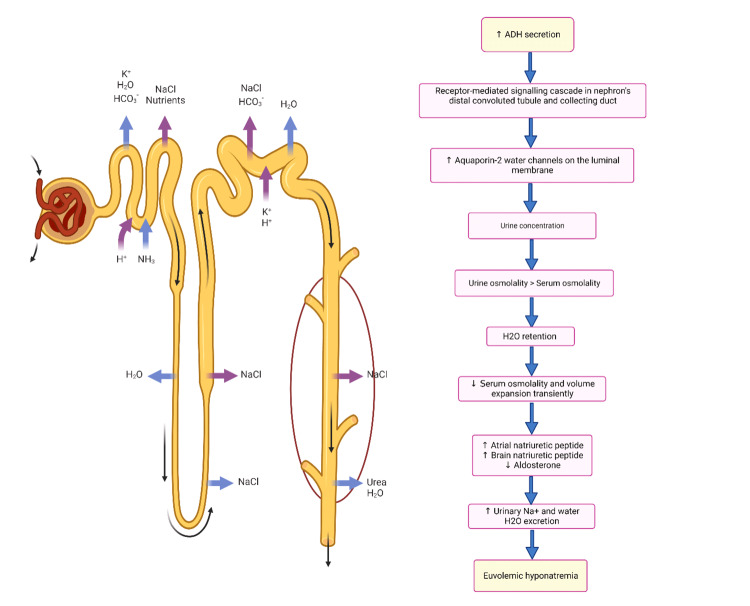
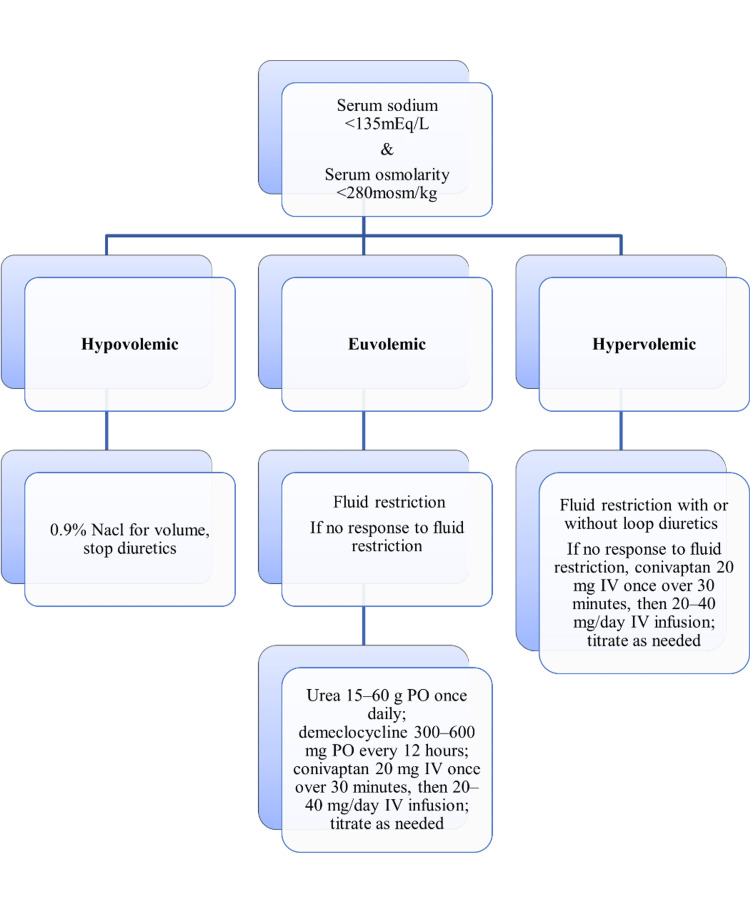
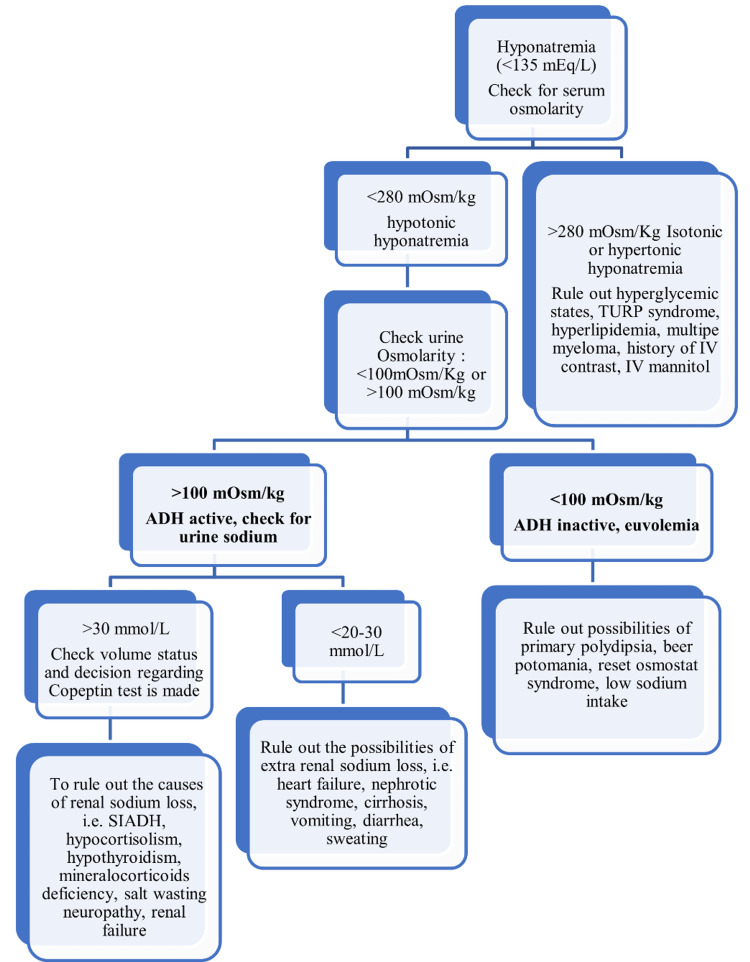
Hyponatremia is the most prevalent electrolyte imbalance encountered among hospitalized patients, athletes, the elderly, patients with chronic ailments, postoperative patients, and a few asymptomatic individuals. Clinical manifestations of hyponatremia can be diverse, with characteristic neurological symptoms. Depending on in-depth medical history, physical examination (including volume status assessment), laboratory investigation, and drug history, patients can be classified broadly as undergoing hypervolemic, euvolemic, or hypovolemic hyponatremia. However, patients with hypervolemic hyponatremia often present with distinctive signs such as edema or ascites, and the clinical presentation of hypovolemic and euvolemic hyponatremia poses significant challenges for clinicians. The convolution in clinical manifestations of patients is due to the varied etiologies of euvolemic hyponatremia, such as syndrome of inappropriate antidiuretic hormone secretion (SIADH), adrenocortical insufficiency, hypothyroidism, psychogenic polydipsia, different classes of drugs (chemotherapeutics, antipsychotics, antidepressants), endurance exercise events, and reset osmostat syndrome (ROS). The management of hyponatremia depends on the rate of hyponatremia onset, duration, severity of symptoms, levels of serum sodium, and underlying comorbidities. Over the last decade, the clinical understanding of hyponatremia has been scattered due to the introduction of innovative laboratory markers and new drugs. This article will be a conspectus of all the recent advancements in the field of diagnosis, investigations, management, and associations of hyponatremia, along with traditional clinical practices. Subsequently, a holistic overview has been laid out for the clinicians to better understand and identify knowledge deficiencies on this topic.
低钠血症是住院患者、运动员、老年人、慢性病患者、术后患者以及少数无症状个体中最常见的电解质失衡情况。低钠血症的临床表现多种多样,具有典型的神经症状。根据详细的病史、体格检查(包括容量状态评估)、实验室检查和用药史,患者可大致分为高容量性、等容量性或低容量性低钠血症。然而,高容量性低钠血症患者常表现出水肿或腹水等独特体征,而低容量性和等容量性低钠血症的临床表现给临床医生带来了重大挑战。患者临床表现的复杂性是由于等容量性低钠血症病因多样,如抗利尿激素分泌不当综合征(SIADH)、肾上腺皮质功能不全、甲状腺功能减退、精神性多饮、不同种类的药物(化疗药物、抗精神病药物、抗抑郁药物)、耐力运动项目以及渗透压调定点重置综合征(ROS)。低钠血症的治疗取决于低钠血症的起病速度、持续时间、症状严重程度、血清钠水平以及基础合并症。在过去十年中,由于引入了创新的实验室指标和新药,对低钠血症的临床认识较为分散。本文将概述低钠血症在诊断、检查、治疗以及相关方面的所有最新进展,以及传统的临床实践。随后,为临床医生提供了一个全面的概述,以便更好地理解和识别该主题上的知识缺陷。