Cardiovascular Institute and Division of Cardiology, Department of Medicine, Beth Israel Deaconess Medical Center, Boston, MA (M.F.R., J.K.P., A.S.P., N.O., D.W., J.E.H.).
Division of Cardiology, Department of Medicine, Massachusetts General Hospital, Boston (E.S.L., J.N.M., R.M., G.D.L.).
Circ Heart Fail. 2023 Nov;16(11):e010618. doi: 10.1161/CIRCHEARTFAILURE.123.010618. Epub 2023 Sep 13.
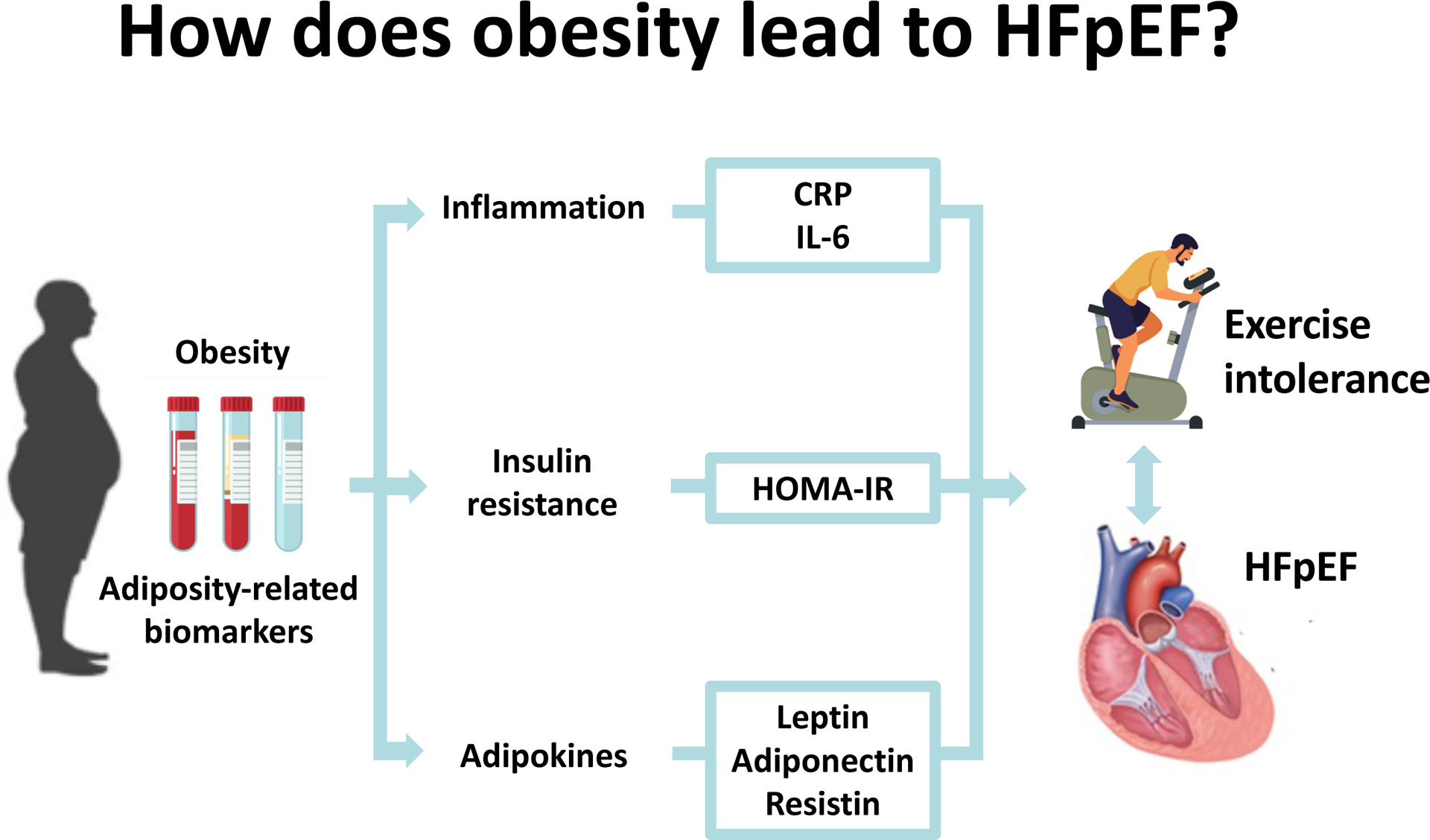
Obesity and adiposity are associated with an increased risk of heart failure with preserved ejection fraction (HFpEF); yet, specific underlying mechanisms remain unclear. We sought to examine the association of obesity-related biomarkers including adipokines (leptin, resistin, adiponectin), inflammatory markers (CRP [C-reactive protein], IL-6 [interleukin-6]), and insulin resistance (HOMA-IR) with HFpEF status, exercise capacity, and cardiovascular outcomes.
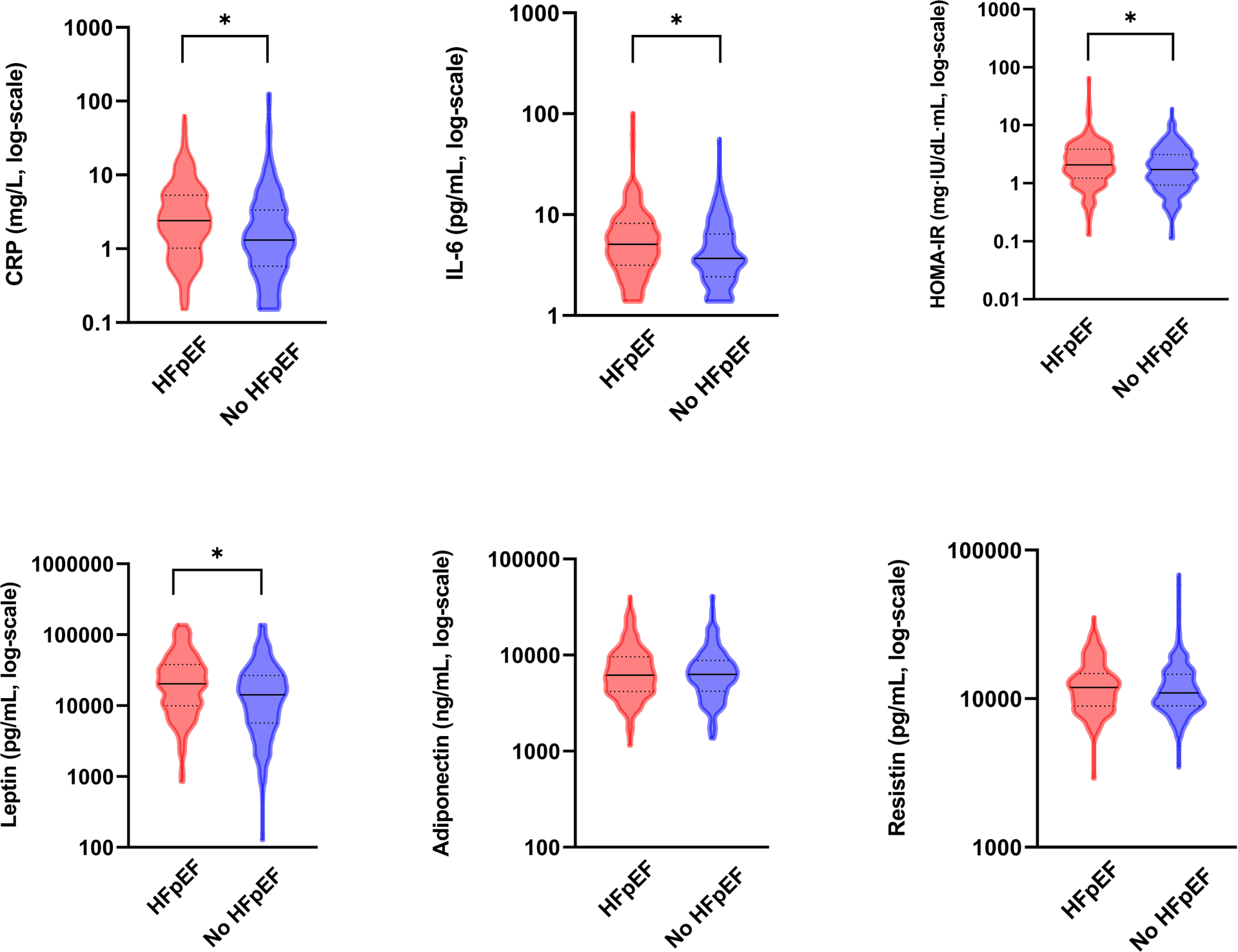
We studied 509 consecutive patients with left ventricular ejection fraction ≥50% and chronic dyspnea, who underwent clinically indicated cardiopulmonary exercise test with invasive hemodynamic monitoring between 2006 and 2017. We defined HFpEF based on the presence of elevated left ventricular filling pressures at rest or during exercise. Fasting blood samples collected at the time of the cardiopulmonary exercise test were used to assay obesity-related biomarkers. We examined the association of log-transformed biomarkers with HFpEF status and exercise traits using multivariable-adjusted logistic regression models.
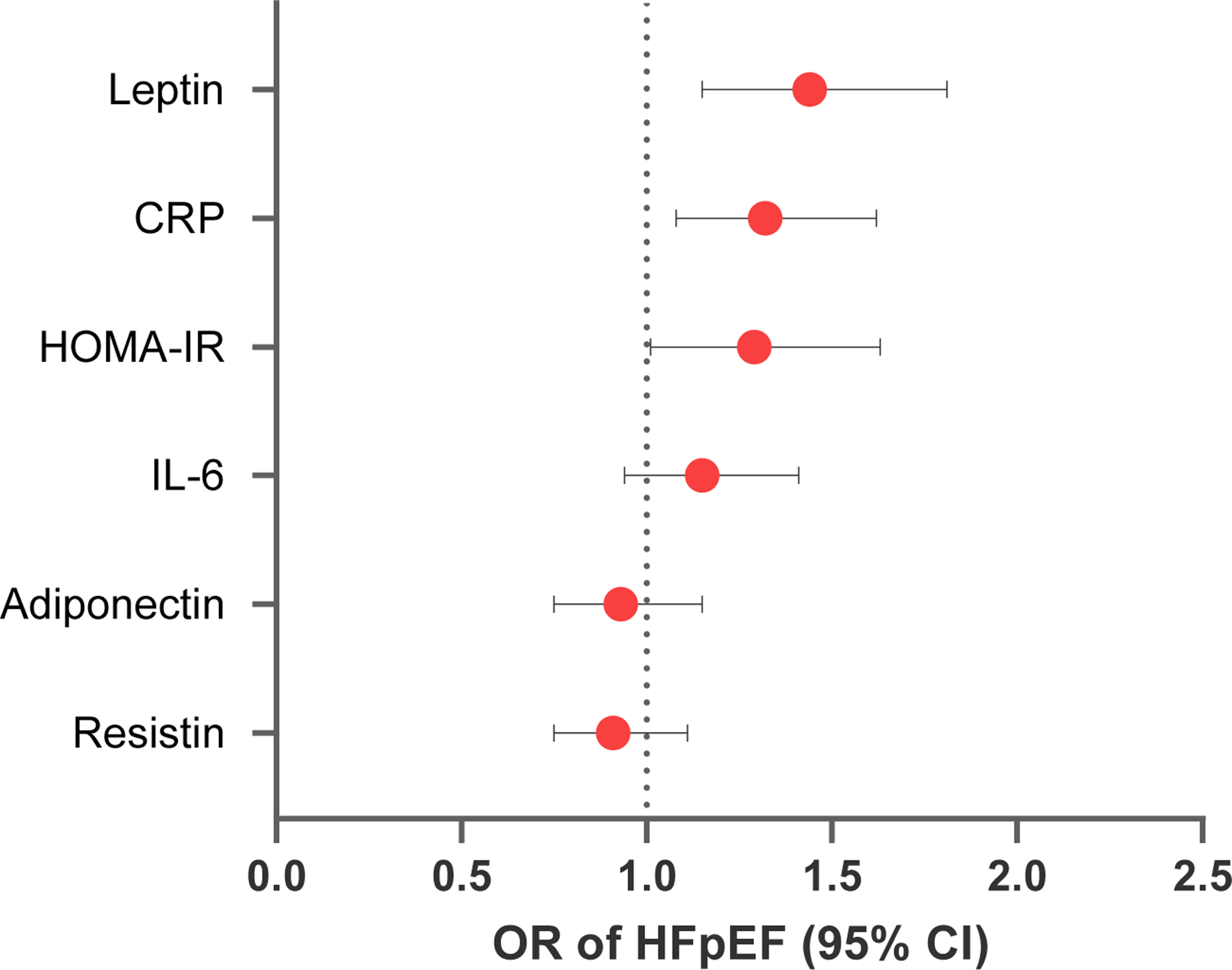
We observed associations of obesity-related biomarkers with measures of impaired exercise capacity including peak VO (≤0.002 for all biomarkers). The largest effect size was seen with leptin, where a 1-SD higher leptin was associated with a 2.35 mL/kg per min lower peak VO (β, -2.35±0.19; <0.001). In addition, specific biomarkers were associated with distinct measures of exercise reserve including blood pressure (homeostatic model assessment of insulin resistance, leptin, adiponectin; ≤0.002 for all), and chronotropic response (CRP, IL-6, homeostatic model assessment of insulin resistance, leptin, and resistin; <0.05 for all). Our findings suggest that among the obesity-related biomarkers studied, higher levels of leptin and CRP are independently associated with increased odds of HFpEF, with odds ratios of 1.36 (95% CI, 1.09-1.70) and 1.25 (95% CI, 1.03-1.52), respectively.
Specific obesity-related pathways including inflammation, adipokine signaling, and insulin resistance may underlie the association of obesity with HFpEF and exercise intolerance.
肥胖和肥胖症与射血分数保留型心力衰竭(HFpEF)的风险增加相关;然而,具体的潜在机制仍不清楚。我们试图研究肥胖相关生物标志物(包括 adipokines[瘦素、抵抗素、脂联素]、炎症标志物[C 反应蛋白(CRP)、白细胞介素-6(IL-6)]和胰岛素抵抗(HOMA-IR))与 HFpEF 状态、运动能力和心血管结局的相关性。
我们研究了 2006 年至 2017 年间因慢性呼吸困难接受临床指征心肺运动试验(CPET)并进行有创血流动力学监测的 509 例左心室射血分数≥50%的连续患者。我们根据静息或运动时左心室充盈压升高来定义 HFpEF。CPET 时采集的空腹血样用于检测肥胖相关生物标志物。我们使用多变量调整的逻辑回归模型来研究 log 转换生物标志物与 HFpEF 状态和运动特征的相关性。
我们观察到肥胖相关生物标志物与运动能力受损的指标相关,包括峰值 VO(所有生物标志物均≤0.002)。最大的效应大小见于瘦素,其中瘦素每增加 1 个标准差,峰值 VO 降低 2.35mL/kg/min(β,-2.35±0.19;<0.001)。此外,特定的生物标志物与不同的运动储备指标相关,包括血压(稳态模型评估的胰岛素抵抗、瘦素、脂联素;所有生物标志物均≤0.002)和变时反应(CRP、IL-6、稳态模型评估的胰岛素抵抗、瘦素和抵抗素;所有生物标志物均<0.05)。我们的研究结果表明,在所研究的肥胖相关生物标志物中,较高的瘦素和 CRP 水平与 HFpEF 的发生几率增加独立相关,比值比分别为 1.36(95%CI,1.09-1.70)和 1.25(95%CI,1.03-1.52)。
特定的肥胖相关途径,包括炎症、 adipokine 信号和胰岛素抵抗,可能是肥胖与 HFpEF 和运动不耐受相关的基础。