Lawton Beverley, MacDonald Evelyn Jane, Storey Francesca, Stanton Jo-Ann, Adcock Anna, Gibson Melanie, Parag Varsha, Sparkes Ngaire Kereru, Kaimoana Bobby, King Frances, Terry Marion, Watson Huti, Bennett Matthew, Lambert Charles Seymour, Geller Stacie, Paasi Isitokia, Hibma Merilyn, Sykes Peter, Hawkes David, Saville Marion
National Women's Health Research Centre, Faculty of Health, Victoria University of Wellington, Wellington, New Zealand.
National Institute for Health Innovation, School of Population Health, University of Auckland, Auckland, New Zealand.
JMIR Res Protoc. 2023 Sep 14;12:e51643. doi: 10.2196/51643.
Māori are the Indigenous people of Aotearoa (New Zealand). Despite global acceptance that cervical cancer is almost entirely preventable through vaccination and screening, wāhine Māori (Māori women) are more likely to have cervical cancer and 2.5 times more likely to die from it than non-Māori women. Rural Māori residents diagnosed with cervical cancer have worse outcomes than urban residents. Living in rural Aotearoa means experiencing barriers to appropriate and timely health care, resulting from distance, the lack of community resourcing, and low prioritization of rural needs by the health system and government. These barriers are compounded by the current screening processes and referral pathways that create delays at each step. Screening for high-risk human papillomavirus (hrHPV) and point-of-care (POC) testing are scientific advances used globally to prevent cervical cancer.
This study aims to compare acceptability, feasibility, timeliness, referral to, and attendance for colposcopy following hrHPV detection between a community-controlled pathway and standard care.
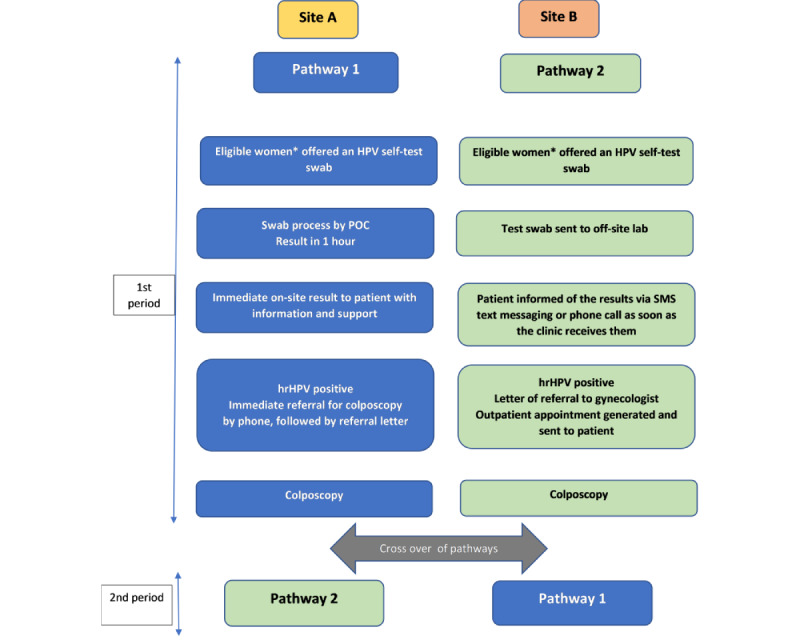
This is a cluster randomized crossover trial, with 2 primary care practices (study sites) as clusters. Each site was randomized to implement either pathway 1 or 2, with crossover occurring at 15 months. Pathway 1 (community-controlled pathway) comprises HPV self-testing, 1-hour POC results, face-to-face information, support, and immediate referral to colposcopy for women with a positive test result. Pathway 2 (standard care) comprises HPV self-testing, laboratory analysis, usual results giving, information, support, and standard referral pathways for women with a positive test result. The primary outcome is the proportion of women with hrHPV-positive results having a colposcopy within 20 working days of the HPV test (national performance indicator). Qualitative research will analyze successes and challenges of both pathways from the perspectives of governance groups, clinical staff, women, and their family. This information will directly inform the new National Cervical Screening Program.
In the first 15-month period, 743 eligible HPV self-tests were performed: 370 in pathway 1 with POC testing and 373 in pathway 2 with laboratory testing. The positivity rate for hrHPV was 7.3% (54/743). Data collection for the second period, qualitative interviews, and analyses are ongoing.
This Māori-centered study combines quantitative and qualitative research to compare 2 clinical pathways from detection of hrHPV to colposcopy. This protocol draws on rural community practices strengths, successfully engaging Māori from a whānau ora (family wellness) approach including kanohi ki te kanohi (face-to-face), kaiāwhina (nonclinical community health workers), and multiple venues for interventions. It will inform the theory and practice of rural models of the use of innovative technology, addressing Māori cervical cancer inequities and facilitating Māori wellness. The findings are anticipated to be applicable to other Indigenous and rural people in high-income countries.
Australian New Zealand Clinical Trials Registry (ANZCTR) ACTRN12621000553875; https://anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12621000553875.
INTERNATIONAL REGISTERED REPORT IDENTIFIER (IRRID): DERR1-10.2196/51643.
毛利人是奥特亚罗瓦(新西兰)的原住民。尽管全球公认宫颈癌几乎完全可以通过疫苗接种和筛查来预防,但毛利女性比非毛利女性更易患宫颈癌,且死于宫颈癌的可能性高出2.5倍。被诊断出患有宫颈癌的农村毛利居民的治疗结果比城市居民更差。生活在新西兰农村意味着面临获得适当和及时医疗保健的障碍,这些障碍源于距离远、社区资源匮乏以及卫生系统和政府对农村需求的低优先级。当前的筛查流程和转诊途径在每个环节都会造成延误,使这些障碍更加复杂。高危型人乳头瘤病毒(hrHPV)筛查和即时检测(POC)是全球用于预防宫颈癌的科学进展。
本研究旨在比较社区控制途径和标准护理在hrHPV检测后阴道镜检查的可接受性、可行性、及时性、转诊情况和就诊率。
这是一项整群随机交叉试验,将2个初级保健机构(研究地点)作为整群。每个地点随机实施途径1或途径2,在15个月时交叉。途径1(社区控制途径)包括HPV自我检测、1小时即时检测结果、面对面信息、支持,并将检测结果呈阳性的女性立即转诊至阴道镜检查。途径2(标准护理)包括HPV自我检测、实验室分析、常规结果告知、信息、支持,并为检测结果呈阳性的女性提供标准转诊途径。主要结局是hrHPV检测结果呈阳性的女性在HPV检测后20个工作日内进行阴道镜检查的比例(国家绩效指标)。定性研究将从管理小组、临床工作人员、女性及其家人的角度分析两种途径的成功经验和挑战。这些信息将直接为新的国家宫颈癌筛查计划提供参考。
在第一个15个月期间,共进行了743次符合条件的HPV自我检测:途径1采用即时检测进行了370次,途径2采用实验室检测进行了373次。hrHPV阳性率为7.3%(54/743)。第二个时期的数据收集、定性访谈和分析正在进行中。
这项以毛利人为中心的研究结合了定量和定性研究,以比较从hrHPV检测到阴道镜检查的两种临床途径。该方案利用了农村社区实践的优势,成功地从毛利人的家庭健康方法(包括面对面交流、非临床社区卫生工作者)以及多个干预场所吸引了毛利人参与。它将为农村创新技术使用模式的理论和实践提供参考,解决毛利人宫颈癌的不平等问题并促进毛利人的健康。研究结果预计将适用于高收入国家的其他原住民和农村人口。
澳大利亚新西兰临床试验注册中心(ANZCTR)ACTRN12621000553875;https://anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12621000553875。
国际注册报告识别码(IRRID):DERR1-10.2196/