Department of Orthopaedic Surgery, Massachusetts General Hospital, Boston, Massachusetts, USA.
Department of Orthopaedic Surgery, University of Nebraska, Omaha, Nebraska, USA.
Am J Sports Med. 2023 Oct;51(12):3268-3279. doi: 10.1177/03635465231197374. Epub 2023 Sep 15.
The overlapping biomechanical relationship between the lumbosacral spine and pelvis poses unique challenges to patients with concomitant pathologies limiting spinopelvic range of motion.
To assess the influence of concomitant, symptomatic lumbosacral spine pathology on patient-reported outcome measures (PROMs) after hip arthroscopy for the treatment of femoroacetabular impingement (FAI) and symptomatic labral tears.
Cohort study; Level of evidence, 3.
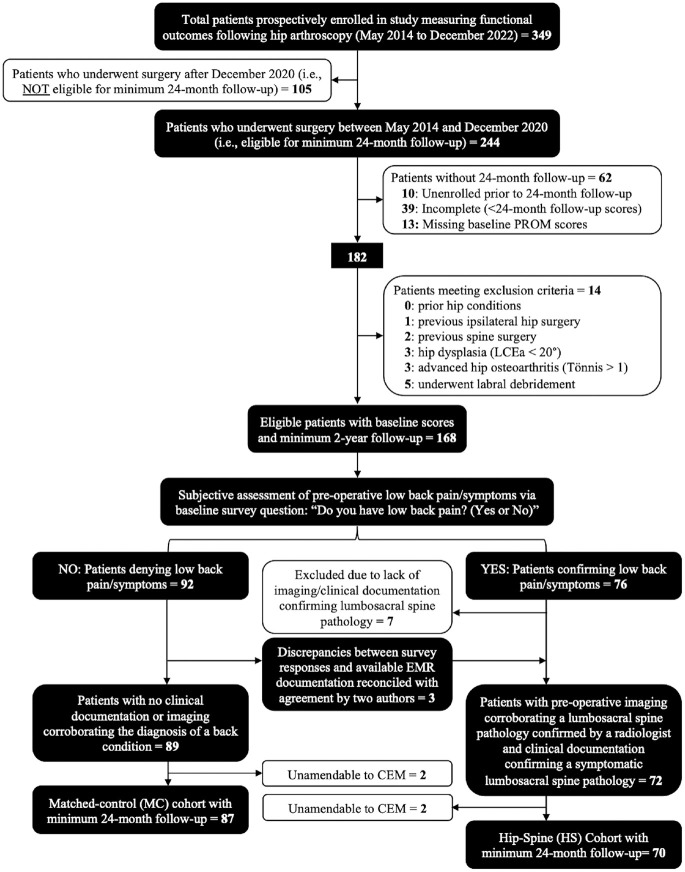
A retrospective query of prospectively collected data identified patients aged ≥18 years with a minimum 24-month follow-up who underwent hip arthroscopy by a single surgeon for the treatment of symptomatic labral tears secondary to FAI. Patients were stratified into cohorts based on the presence (hip-spine [HS]) or absence (matched control [MC]) of symptomatic lumbosacral spine pathology. Inclusion within the HS cohort required confirmation of lower back pain/symptoms on preoperative surveys plus a diagnosis of lumbosacral spine pathology verified by radiology reports and correlating clinical documentation. Patients with previous spine surgery were excluded. PROMs were compared between groups, along with rates of achieving minimal clinically important difference (MCID) thresholds, Patient Acceptable Symptom State (PASS) thresholds, revision arthroscopy, and conversion to total hip arthroplasty (THA).
A total of 70 patients with lumbosacral pathology were coarsened exact matched to 87 control patients without spinal pathology. The HS cohort had preoperative baseline scores that were significantly worse for nearly all PROMs. Follow-ups at 3, 6, 12, and 24 months displayed similar trends, with the HS cohort demonstrating significantly worse scores for most collected outcomes. However, at every time point, HS and MC patients exhibited similar magnitudes of improvement across all PROM and pain metrics. Furthermore, while significantly fewer HS patients achieved PASS for nearly all PROMs at 12- and 24-month follow-ups, MCID thresholds were reached at similar or greater rates across all PROMs relative to the MC cohort. Finally, there were no significant differences in rates of revision or THA between cohorts at maximum available follow-up.
After hip arthroscopy to address labral tears in the setting of FAI, patients with symptomatic lumbosacral pathologies and no history of spine surgery were found to exhibit inferior pre- and postoperative PROMs but achieved statistically similar clinical benefit and rates of PROM improvement through 24-month follow-up compared with the MC cohort with isolated hip disease. These findings aid in providing a realistic recovery timeline and evidence that coexisting hip and spine disorders are not a contraindication for arthroscopic hip preservation surgery.
腰骶脊柱与骨盆之间重叠的生物力学关系给同时患有脊柱和骨盆疾病、限制脊柱骨盆活动度的患者带来了独特的挑战。
评估同时存在症状性腰骶脊柱病变对髋关节镜治疗股骨髋臼撞击症(FAI)和症状性盂唇撕裂患者的患者报告结局测量(PROM)的影响。
队列研究;证据水平,3 级。
对前瞻性收集的数据进行回顾性查询,确定了至少随访 24 个月、由同一位外科医生行髋关节镜治疗的、年龄≥18 岁的患者。根据是否存在(髋关节-脊柱 [HS])或不存在(匹配对照 [MC])症状性腰骶脊柱病变对患者进行分层。HS 队列的纳入标准为术前调查存在下腰痛/症状,且放射学报告和相关临床记录证实存在腰骶脊柱病变。排除既往脊柱手术的患者。比较两组之间的 PROM,并比较达到最小临床重要差异(MCID)阈值、患者可接受的症状状态(PASS)阈值、翻修关节镜和转换为全髋关节置换(THA)的比例。
共对 70 例存在腰骶病变的患者进行了粗略精确匹配,以匹配 87 例无脊柱病变的对照患者。HS 组在几乎所有 PROM 的术前基线评分都明显更差。在 3、6、12 和 24 个月的随访中,出现了类似的趋势,HS 组在大多数收集的结果中显示出明显更差的评分。然而,在每个时间点,HS 和 MC 患者在所有 PROM 和疼痛指标上都表现出相似程度的改善。此外,虽然 HS 患者在 12 和 24 个月的随访中几乎所有 PROM 的 PASS 率都明显较低,但 MCID 阈值在所有 PROM 中达到的比例相似或更高,与 MC 组相比。最后,在可获得的最大随访中,两组之间的翻修或 THA 率没有显著差异。
在髋关节镜治疗 FA I 合并症状性腰骶脊柱病变和无脊柱手术史的患者中,发现术前和术后 PROM 明显较差,但与仅患有髋关节疾病的 MC 组相比,通过 24 个月的随访,在统计学上达到了相似的临床获益和 PROM 改善率。这些发现有助于提供现实的恢复时间表,并证明共存的髋关节和脊柱疾病不是关节镜髋关节保存手术的禁忌症。