Department of Internal Medicine, Clinic of Cardiology, George Emil Palade University of Medicine, Pharmacy, Science and Technology, Targu Mures, Romania.
County Clinical Emergency Hospital Targu Mures, Targu Mures, Romania.
Diabetes Care. 2023 Nov 1;46(11):2015-2023. doi: 10.2337/dc23-0710.
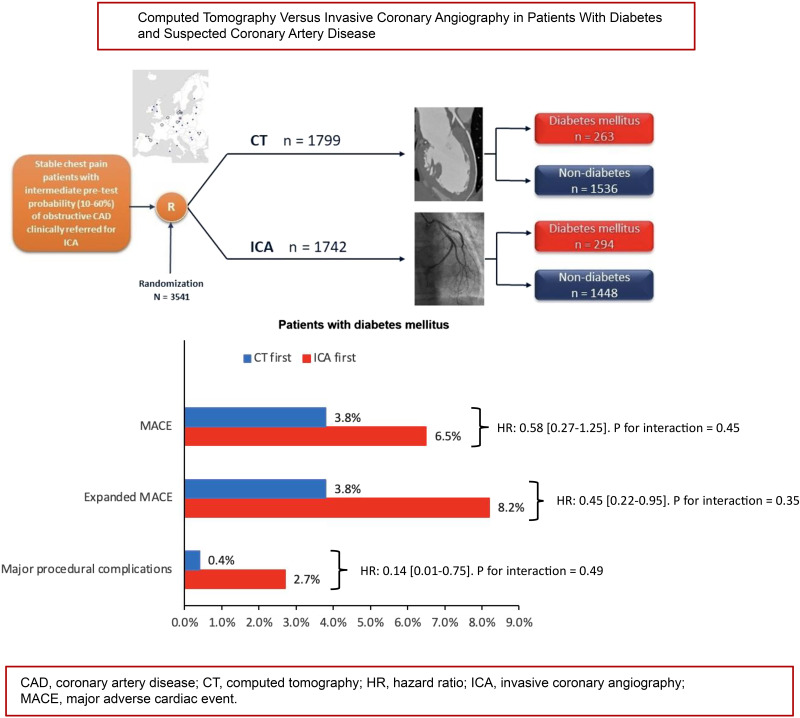
To compare cardiac computed tomography (CT) with invasive coronary angiography (ICA) as the initial strategy in patients with diabetes and stable chest pain.
This prespecified analysis of the multicenter DISCHARGE trial in 16 European countries was performed in patients with stable chest pain and intermediate pretest probability of coronary artery disease. The primary end point was a major adverse cardiac event (MACE) (cardiovascular death, nonfatal myocardial infarction, or stroke), and the secondary end point was expanded MACE (including transient ischemic attacks and major procedure-related complications).
Follow-up at a median of 3.5 years was available in 3,541 patients of whom 557 (CT group n = 263 vs. ICA group n = 294) had diabetes and 2,984 (CT group n = 1,536 vs. ICA group n = 1,448) did not. No statistically significant diabetes interaction was found for MACE (P = 0.45), expanded MACE (P = 0.35), or major procedure-related complications (P = 0.49). In both patients with and without diabetes, the rate of MACE did not differ between CT and ICA groups. In patients with diabetes, the expanded MACE end point occurred less frequently in the CT group than in the ICA group (3.8% [10 of 263] vs. 8.2% [24 of 294], hazard ratio [HR] 0.45 [95% CI 0.22-0.95]), as did the major procedure-related complication rate (0.4% [1 of 263] vs. 2.7% [8 of 294], HR 0.30 [95% CI 0.13 - 0.63]).
In patients with diabetes referred for ICA for the investigation of stable chest pain, a CT-first strategy compared with an ICA-first strategy showed no difference in MACE and may potentially be associated with a lower rate of expanded MACE and major procedure-related complications.
比较心脏计算机断层扫描(CT)与有创性冠状动脉造影(ICA)作为糖尿病合并稳定型胸痛患者的初始策略。
本研究为多中心 DISCHARGE 试验的预设分析,纳入了 16 个欧洲国家的稳定型胸痛且有中等程度冠状动脉疾病预测值的患者。主要终点为主要不良心脏事件(MACE)(心血管死亡、非致死性心肌梗死或卒中),次要终点为扩大 MACE(包括短暂性脑缺血发作和主要操作相关并发症)。
中位随访 3.5 年,3541 例患者中 557 例(CT 组 n = 263 例,ICA 组 n = 294 例)患有糖尿病,2984 例(CT 组 n = 1536 例,ICA 组 n = 1448 例)无糖尿病。MACE(P = 0.45)、扩大 MACE(P = 0.35)和主要操作相关并发症(P = 0.49)均未发现统计学意义上的糖尿病交互作用。在有或无糖尿病的患者中,CT 与 ICA 组之间的 MACE 发生率均无差异。在糖尿病患者中,CT 组的扩大 MACE 终点发生率低于 ICA 组(3.8%[263 例中的 10 例]比 8.2%[294 例中的 24 例],风险比[HR]0.45[95%可信区间 0.22-0.95]),主要操作相关并发症发生率也较低(0.4%[263 例中的 1 例]比 2.7%[294 例中的 8 例],HR 0.30[95%可信区间 0.13-0.63])。
对于因稳定型胸痛而接受 ICA 检查的糖尿病患者,CT 优先策略与 ICA 优先策略相比,在 MACE 方面无差异,并且可能与扩大 MACE 和主要操作相关并发症的发生率较低相关。