van de Vijver Willem R, Hennecken Jasper, Lagogiannis Ioannis, Pérez Del Villar Candelas, Herrera Cristian, Douek Philippe C, Segev Amit, Hovingh G Kees, Išgum Ivana, Winter Michiel M, Planken R Nils, Claessen Bimmer E P M
Department of Cardiology, Heart Center, Amsterdam University Medical Centers, University of Amsterdam, 1105 AZ Amsterdam, The Netherlands.
Cardiology Centers of the Netherlands, 3544 AD Utrecht, The Netherlands.
Rev Cardiovasc Med. 2024 Dec 17;25(12):442. doi: 10.31083/j.rcm2512442. eCollection 2024 Dec.
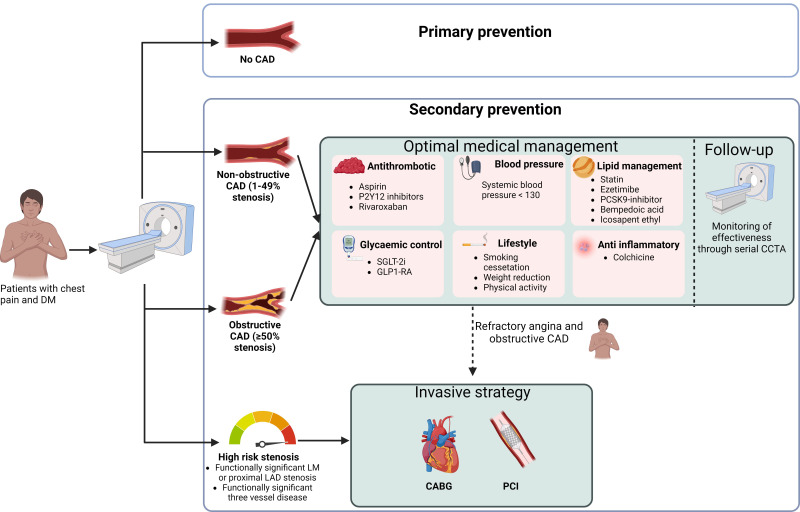
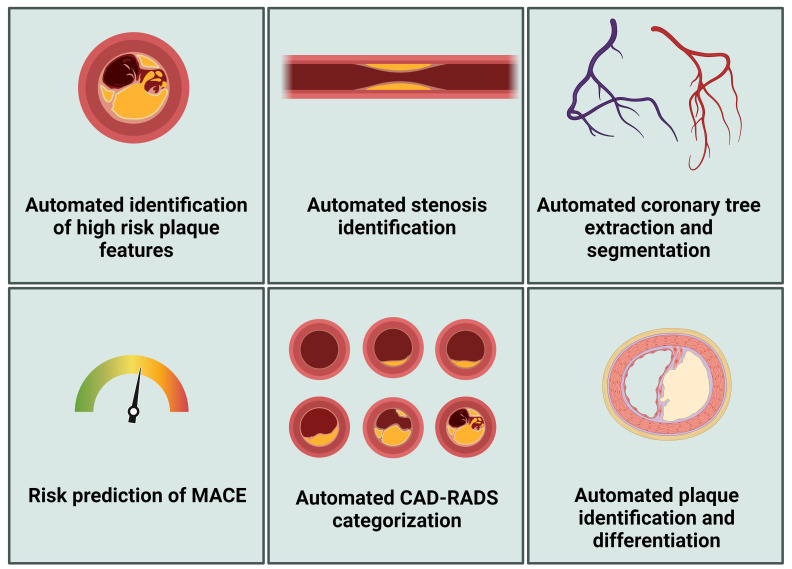
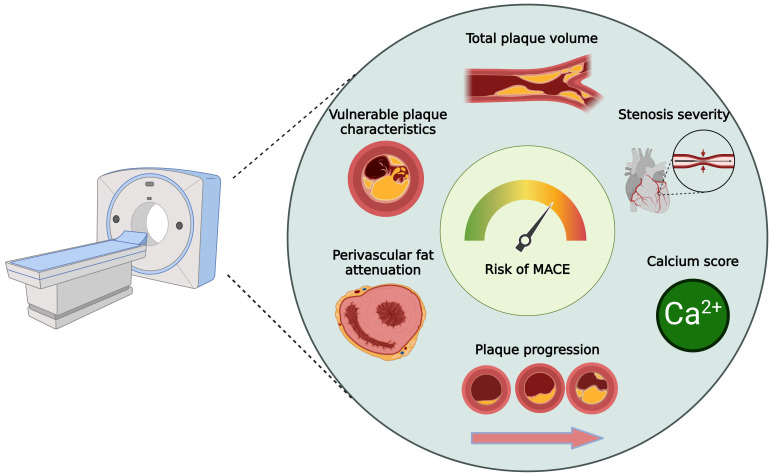
Coronary artery disease (CAD) affects over 200 million individuals globally, accounting for approximately 9 million deaths annually. Patients living with diabetes mellitus exhibit an up to fourfold increased risk of developing CAD compared to individuals without diabetes. Furthermore, CAD is responsible for 40 to 80 percent of the observed mortality rates among patients with type 2 diabetes. Patients with diabetes typically present with non-specific clinical complaints in the setting of myocardial ischemia, and as such, it is critical to select appropriate diagnostic tests to identify those at risk for major adverse cardiac events (MACEs) and for determining optimal management strategies. Studies indicate that patients with diabetes often exhibit more advanced atherosclerosis, a higher calcified plaque burden, and smaller epicardial vessels. The diagnostic performance of coronary computed tomographic angiography (CCTA) in identifying significant stenosis is well-established, and as such, CCTA has been incorporated into current clinical guidelines. However, the predictive accuracy of obstructive CAD in patients with diabetes has been less extensively characterized. CCTA provides detailed insights into coronary anatomy, plaque burden, epicardial vessel stenosis, high-risk plaque features, and other features associated with a higher incidence of MACEs. Recent evidence supports the efficacy of CCTA in diagnosing CAD and improving patient outcomes, leading to its recommendation as a primary diagnostic tool for stable angina and risk stratification. However, its specific benefits in patients with diabetes require further elucidation. This review examines several key aspects of the utility of CCTA in patients with diabetes: (i) the diagnostic accuracy of CCTA in detecting obstructive CAD, (ii) the effect of CCTA as a first-line test for individualized risk stratification for cardiovascular outcomes, (iii) its role in guiding therapeutic management, and (iv) future perspectives in risk stratification and the role of artificial intelligence.
冠状动脉疾病(CAD)在全球影响着超过2亿人,每年导致约900万人死亡。与非糖尿病患者相比,糖尿病患者患CAD的风险增加了四倍。此外,CAD导致2型糖尿病患者中40%至80%的观察到的死亡率。糖尿病患者在心肌缺血时通常表现为非特异性临床症状,因此,选择合适的诊断测试以识别有重大不良心脏事件(MACE)风险的患者并确定最佳管理策略至关重要。研究表明,糖尿病患者通常表现出更严重的动脉粥样硬化、更高的钙化斑块负荷和更小的心外膜血管。冠状动脉计算机断层扫描血管造影(CCTA)在识别显著狭窄方面的诊断性能已得到充分证实,因此,CCTA已被纳入当前临床指南。然而,糖尿病患者中阻塞性CAD的预测准确性尚未得到广泛研究。CCTA提供了关于冠状动脉解剖结构、斑块负荷、心外膜血管狭窄、高危斑块特征以及与MACE发生率较高相关的其他特征的详细信息。最近的证据支持CCTA在诊断CAD和改善患者预后方面的有效性,导致其被推荐为稳定型心绞痛和风险分层的主要诊断工具。然而,其在糖尿病患者中的具体益处需要进一步阐明。本综述探讨了CCTA在糖尿病患者中的几个关键应用方面:(i)CCTA检测阻塞性CAD的诊断准确性,(ii)CCTA作为心血管结局个体化风险分层的一线测试的效果,(iii)其在指导治疗管理中的作用,以及(iv)风险分层的未来展望和人工智能的作用。