Multidisciplinary Oncology and Therapeutic Innovations Department, Aix Marseille Univ, APHM, INSERM, CNRS, CRCM, Hôpital Nord, Marseille, France.
Centre de Recherche en Cancérologie de Marseille (CRCM), INSERM UMR1068, CNRS UMR725, Laboratoire d'Oncologie Prédictive, Aix Marseille Univ, Marseille, France.
J Transl Med. 2023 Sep 19;21(1):637. doi: 10.1186/s12967-023-04463-2.
Anti-PD1/PDL1 immune checkpoint inhibitors (ICI) transformed the prognosis of patients with advanced non-small cell lung cancer (NSCLC). However, the response rate remains disappointing and toxicity may be life-threatening, making urgent identification of biomarkers predictive for efficacy. Immunologic Constant of Rejection signature (ICR) is a 20-gene expression signature of cytotoxic immune response with prognostic value in some solid cancers. Our objective was to assess its predictive value for benefit from anti-PD1/PDL1 in patients with advanced NSCLC.
We retrospectively profiled 44 primary tumors derived from NSCLC patients treated with ICI as single-agent in at least the second-line metastatic setting. Transcriptomic analysis was performed using the nCounter analysis system and the PanCancer Immune Profiling Panel. We then pooled our data with clinico-biological data from four public gene expression data sets, leading to a total of 162 NSCLC patients treated with single-agent anti-PD1/PDL1. ICR was applied to all samples and correlation was searched between ICR classes and the Durable Clinical Benefit (DCB), defined as stable disease or objective response according to RECIST 1.1 for a minimum of 6 months after the start of ICI.
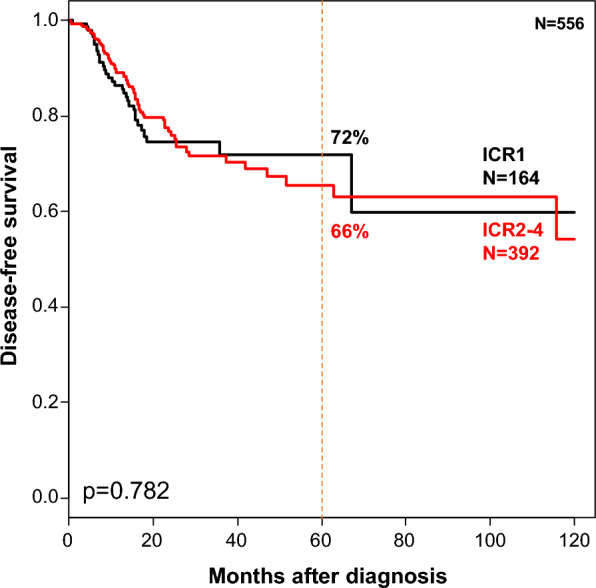
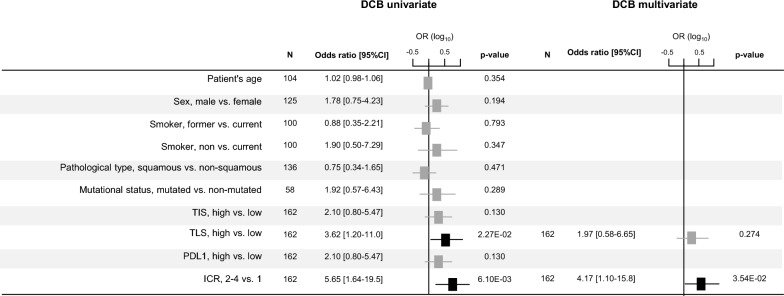
The DCB rate was 29%; 22% of samples were classified as ICR1, 30% ICR2, 22% ICR3, and 26% ICR4. These classes were not associated with the clinico-pathological variables, but showed enrichment from ICR1 to ICR4 in quantitative/qualitative markers of immune response. ICR2-4 class was associated with a 5.65-fold DCB rate when compared with ICR1 class. In multivariate analysis, ICR classification remained associated with DCB, independently from PDL1 expression and other predictive immune signatures. By contrast, it was not associated with disease-free survival in 556 NSCLC TCGA patients untreated with ICI.
The 20-gene ICR signature was independently associated with benefit from anti-PD1/PDL1 ICI in patients with advanced NSCLC. Validation in larger retrospective and prospective series is warranted.
抗 PD-1/PD-L1 免疫检查点抑制剂(ICI)改变了晚期非小细胞肺癌(NSCLC)患者的预后。然而,反应率仍然不尽如人意,毒性可能危及生命,因此迫切需要确定预测疗效的生物标志物。免疫排斥常数(ICR)是一种 20 基因表达的细胞毒性免疫反应标志物,在一些实体瘤中具有预后价值。我们的目的是评估其在接受晚期 NSCLC 患者接受抗 PD-1/PD-L1 单药治疗中的预测价值。
我们回顾性分析了 44 例接受 ICI 单药治疗至少二线转移性晚期 NSCLC 患者的原发肿瘤。使用 nCounter 分析系统和 PanCancer Immune Profiling 面板进行转录组分析。然后,我们将我们的数据与来自四个公共基因表达数据集的临床生物学数据进行了汇总,总共纳入了 162 例接受单药抗 PD-1/PD-L1 治疗的 NSCLC 患者。对所有样本应用 ICR,并在 ICR 分类和持久临床获益(DCB)之间进行了相关性搜索,DCB 定义为根据 RECIST 1.1 在 ICI 开始后至少 6 个月稳定疾病或客观缓解。
DCB 率为 29%;22%的样本为 ICR1 类,30%为 ICR2 类,22%为 ICR3 类,26%为 ICR4 类。这些分类与临床病理变量无关,但在免疫反应的定量/定性标志物中,从 ICR1 到 ICR4 有富集。与 ICR1 类相比,ICR2-4 类的 DCB 率为 5.65 倍。多变量分析表明,ICR 分类与 DCB 相关,与 PDL1 表达和其他预测性免疫标志物无关。相比之下,在未经 ICI 治疗的 556 例 NSCLC TCGA 患者中,它与无疾病生存无关。
20 基因 ICR 标志物与晚期 NSCLC 患者接受抗 PD-1/PD-L1 ICI 治疗的获益独立相关。需要在更大的回顾性和前瞻性系列中进行验证。