Department of Cancer Immunology and Virology, Dana-Farber Cancer Institute, Boston, Massachusetts.
Department of Immunology, Harvard Medical School, Boston, Massachusetts.
Clin Cancer Res. 2024 Feb 1;30(3):542-553. doi: 10.1158/1078-0432.CCR-23-1444.
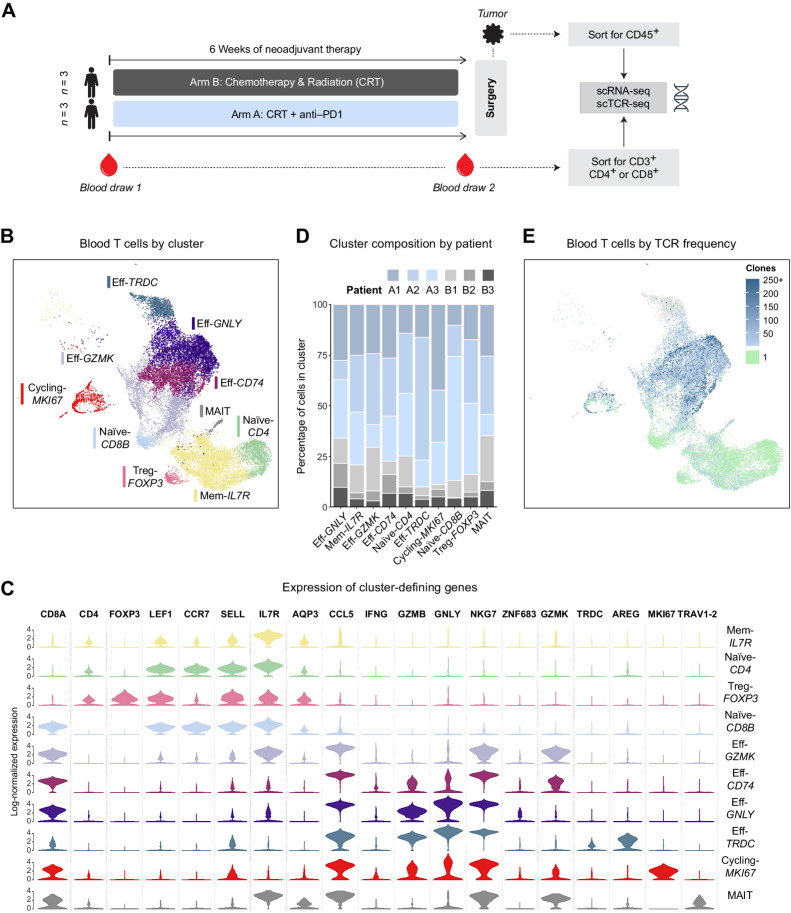
Pancreatic ductal adenocarcinoma (PDAC) trials have evaluated CTLA-4 and/or PD-(L)1 blockade in patients with advanced disease in which bulky tumor burden and limited time to develop antitumor T cells may have contributed to poor clinical efficacy. Here, we evaluated peripheral blood and tumor T cells from patients with PDAC receiving neoadjuvant chemoradiation plus anti-PD-1 (pembrolizumab) versus chemoradiation alone. We analyzed whether PD-1 blockade successfully reactivated T cells in the blood and/or tumor to determine whether lack of clinical benefit could be explained by lack of reactivated T cells versus other factors.
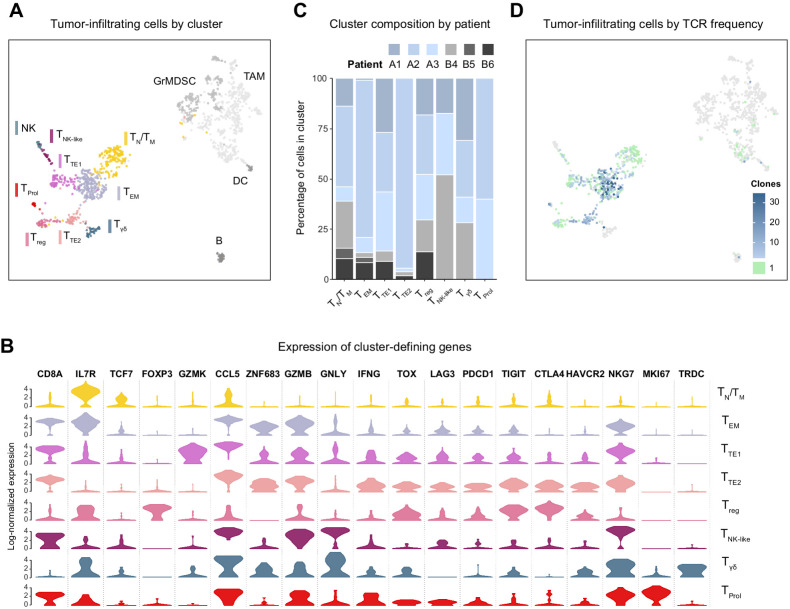
We used single-cell transcriptional profiling and TCR clonotype tracking to identify TCR clonotypes from blood that match clonotypes in the tumor.
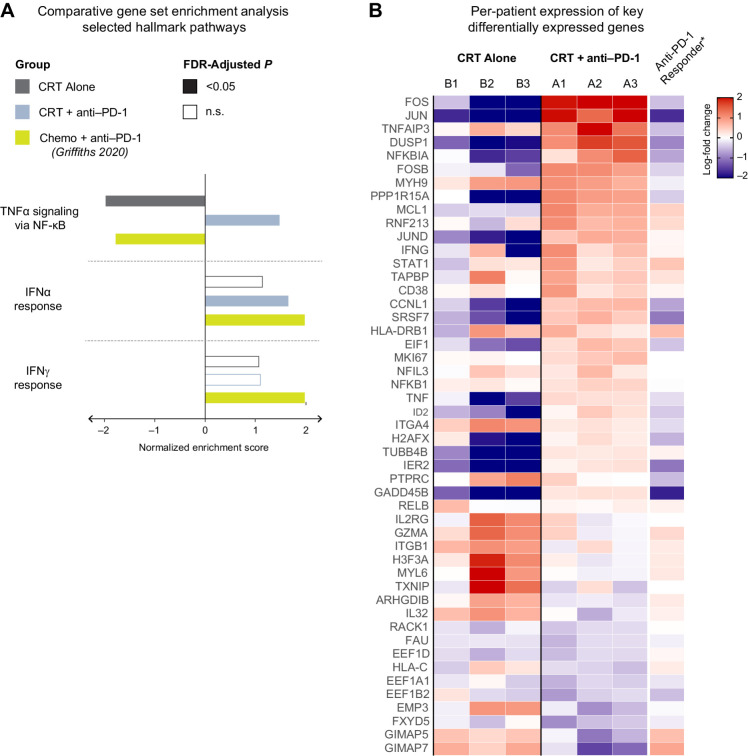
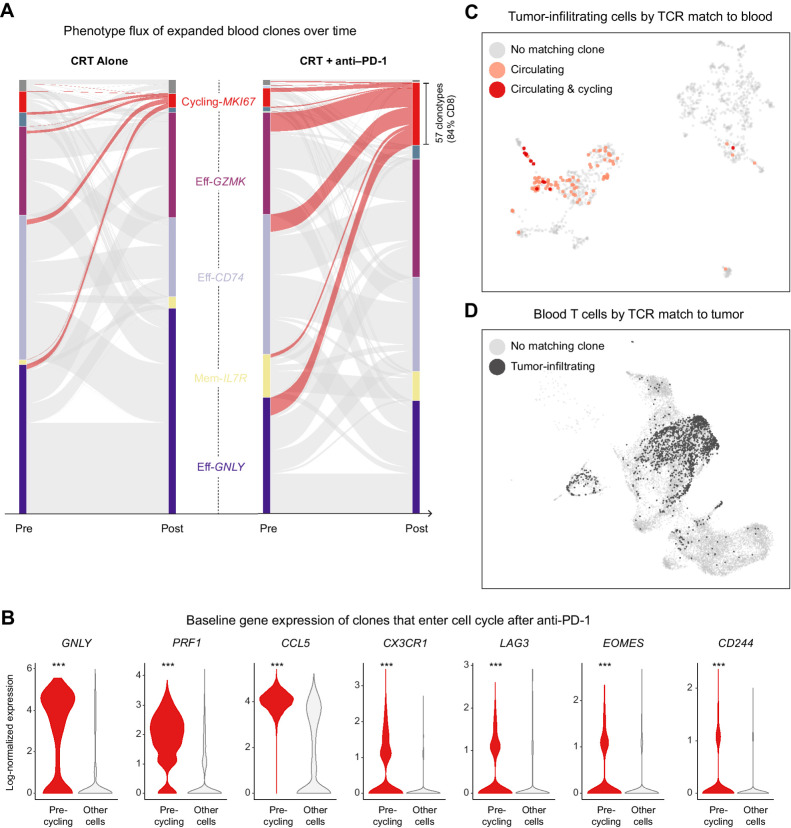
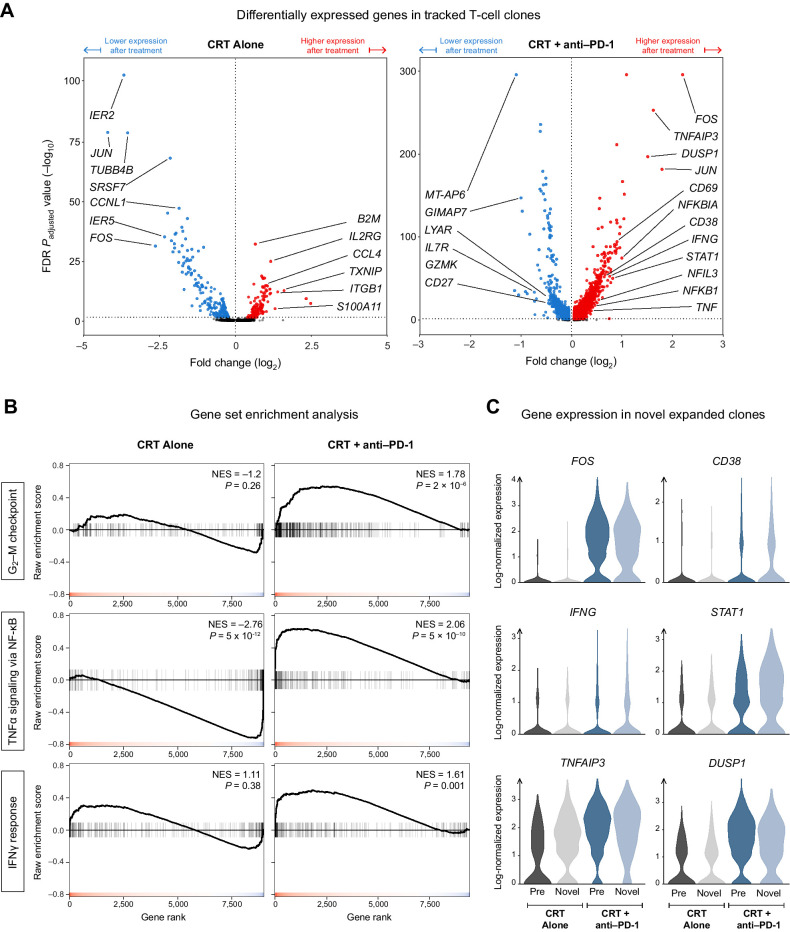
PD-1 blockade increases the flux of TCR clonotypes entering cell cycle and induces an IFNγ signature like that seen in patients with other GI malignancies who respond to PD-1 blockade. However, these reactivated T cells have a robust signature of NF-κB signaling not seen in cases of PD-1 antibody response. Among paired samples between blood and tumor, several of the newly cycling clonotypes matched activated T-cell clonotypes observed in the tumor.
Cytotoxic T cells in the blood of patients with PDAC remain sensitive to reinvigoration by PD-1 blockade, and some have tumor-recognizing potential. Although these T cells proliferate and have a signature of IFN exposure, they also upregulate NF-κB signaling, which potentially counteracts the beneficial effects of anti-PD-1 reinvigoration and marks these T cells as non-productive contributors to antitumor immunity. See related commentary by Lander and DeNardo, p. 474.
在晚期胰腺导管腺癌 (PDAC) 患者中,临床试验评估了 CTLA-4 和/或 PD-(L)1 阻断,在这些患者中,肿瘤负荷大且产生抗肿瘤 T 细胞的时间有限,这可能导致临床疗效不佳。在这里,我们评估了接受新辅助放化疗加抗 PD-1(pembrolizumab)与单纯放化疗的 PDAC 患者的外周血和肿瘤 T 细胞。我们分析了 PD-1 阻断是否成功地在血液和/或肿瘤中重新激活 T 细胞,以确定缺乏临床获益是否可以用缺乏重新激活的 T 细胞来解释,还是其他因素。
我们使用单细胞转录组谱分析和 TCR 克隆型跟踪来鉴定来自血液的与肿瘤中克隆型匹配的 TCR 克隆型。
PD-1 阻断增加了进入细胞周期的 TCR 克隆型的通量,并诱导了一种 IFNγ 特征,类似于其他对 PD-1 阻断有反应的 GI 恶性肿瘤患者的特征。然而,这些重新激活的 T 细胞具有 NF-κB 信号的强烈特征,而在 PD-1 抗体反应的情况下则没有观察到。在血液和肿瘤之间的配对样本中,几个新循环的克隆型与肿瘤中观察到的激活 T 细胞克隆型相匹配。
PDAC 患者血液中的细胞毒性 T 细胞仍然对 PD-1 阻断的再激活敏感,并且其中一些具有识别肿瘤的潜力。尽管这些 T 细胞增殖并具有 IFN 暴露的特征,但它们也上调 NF-κB 信号,这可能抵消了抗 PD-1 再激活的有益效果,并将这些 T 细胞标记为抗肿瘤免疫的非生产性贡献者。请参阅 Lander 和 DeNardo 的相关评论,第 474 页。