Nakagawa Yoichi, Uchida Hiroo, Hinoki Akinari, Shirota Chiyoe, Sumida Wataru, Makita Satoshi, Yokota Kazuki, Amano Hizuru, Yasui Akihiro, Kato Daiki, Gohda Yousuke, Maeda Takuya
Department of Pediatric Surgery, Nagoya University Graduate School of Medicine, 65 Tsurumai-cho, Showa-ku, Nagoya, Aichi, 466-8550, Japan.
Department of Rare/Intractable Cancer Analysis Research, Nagoya University Graduate School of Medicine, 65 Tsurumai-cho, Showa-ku, Nagoya, Aichi, 466-8550, Japan.
Surg Case Rep. 2023 Sep 22;9(1):169. doi: 10.1186/s40792-023-01754-0.
An esophageal anastomotic stricture (EAS) after an esophageal atresia surgery occurs in approximately 4-60% of the cases, and its first-line therapy includes balloon dilatation. Oral balloon dilatation cannot be performed in some EAS cases; conversely, even if dilatation is possible, these strictures recur in some cases, necessitating a surgical procedure for repairing the stenosis. However, these procedures are invasive and have short- and long-term complications. If an EAS recurs repeatedly after multiple balloon dilations, gastroesophageal reflux disease (GERD) may be the underlying cause. A fundoplication procedure may be effective for treating a refractory EAS, as in the present case.
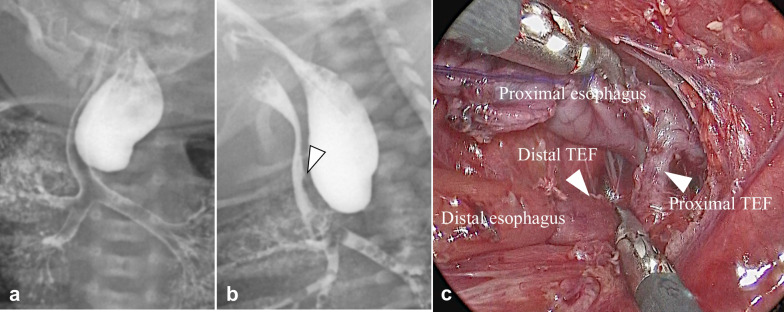
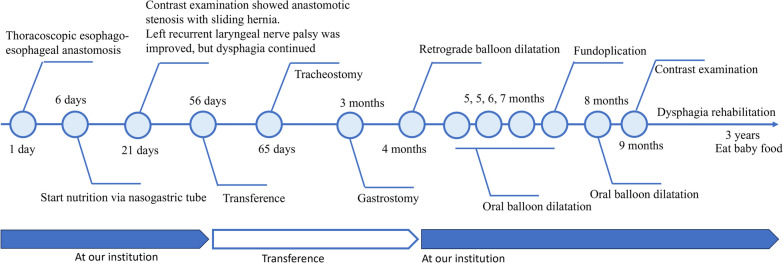
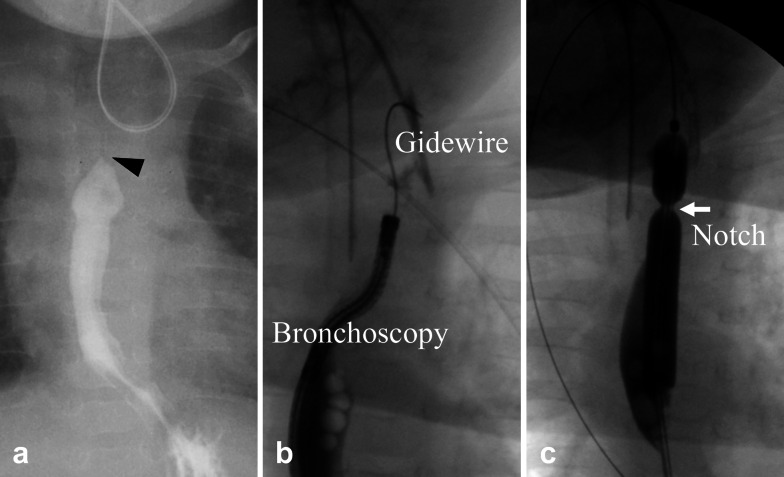
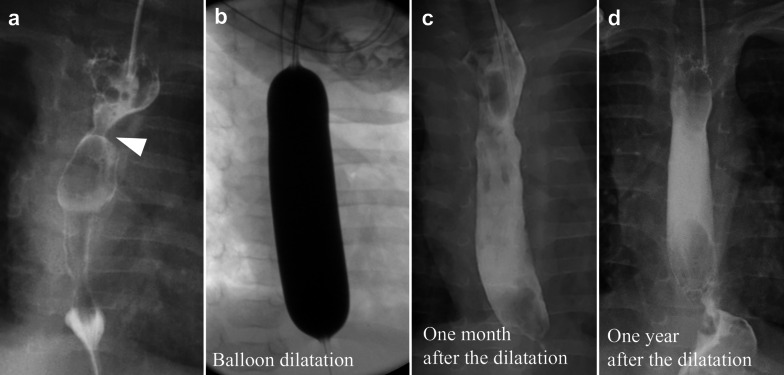
A neonatal patient with type D esophageal atresia underwent thoracoscopic esophago-esophageal anastomosis at the age of 1 day, and her postoperative course was uneventful. Thereafter, the patient underwent gastrostomy for poor oral intake at the age of 3 months. After gastrostomy, the patient presented with a complete obstructive EAS. Balloon dilatation via the oral route was attempted; however, a guidewire could not be inserted into the EAS site. Hence, retrograde balloon dilatation via gastrostomy was performed successfully. However, the EAS recurred easily thereafter, and laparoscopic anti-reflux surgery was performed to prevent GERD. The anti-reflux surgery cured the otherwise refractory EAS and prevented its recurrence.
Retrograde balloon dilatation is another treatment option for an EAS. When an EAS recurs soon after dilatation, the patient must be evaluated for GERD; if severe GERD is observed, an appropriate anti-reflux surgery is required before dilating the EAS.
食管闭锁手术后食管吻合口狭窄(EAS)的发生率约为4% - 60%,其一线治疗方法包括球囊扩张。在一些EAS病例中无法进行经口球囊扩张;相反,即使可以进行扩张,这些狭窄在某些情况下仍会复发,需要进行手术修复狭窄。然而,这些手术具有侵入性,并且存在短期和长期并发症。如果在多次球囊扩张后EAS反复复发,胃食管反流病(GERD)可能是潜在原因。如本病例所示,胃底折叠术可能对治疗难治性EAS有效。
一名患有D型食管闭锁的新生儿在出生1天时接受了胸腔镜下食管 - 食管吻合术,术后恢复顺利。此后,患者在3个月大时因经口摄入不良接受了胃造口术。胃造口术后,患者出现了完全梗阻性EAS。尝试经口途径进行球囊扩张;然而,导丝无法插入EAS部位。因此,成功地通过胃造口术进行了逆行球囊扩张。然而,此后EAS很容易复发,于是进行了腹腔镜抗反流手术以预防GERD。抗反流手术治愈了原本难治的EAS并防止了其复发。
逆行球囊扩张是EAS的另一种治疗选择。当EAS在扩张后很快复发时,必须对患者进行GERD评估;如果观察到严重GERD,则在扩张EAS之前需要进行适当的抗反流手术。