Yamasaki Yasushi, Ozawa Soji, Oguma Junya, Kazuno Akihito, Ninomiya Yamato
Department of Gastroenterological Surgery, Tokai University School of Medicine, 143 Shimokasuya, Isehara, Kanagawa, 259-1193, Japan.
Surg Case Rep. 2016 Dec;2(1):64. doi: 10.1186/s40792-016-0190-1. Epub 2016 Jun 25.
Most of benign esophageal strictures caused by gastroesophageal reflux are short segments and can be treated by an endoscopic dilatation, but cases of long-segment stenosis requiring an esophagectomy are rare.
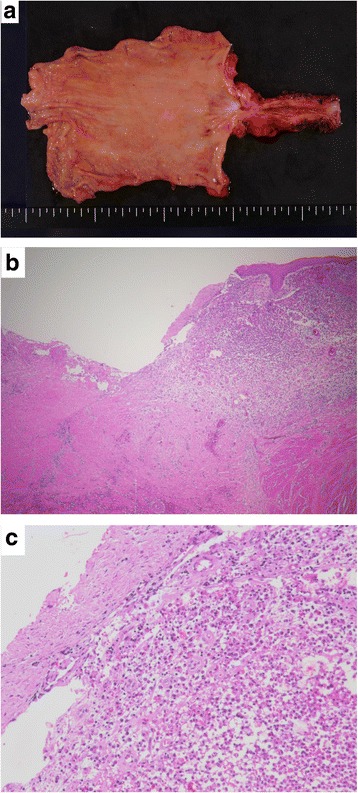
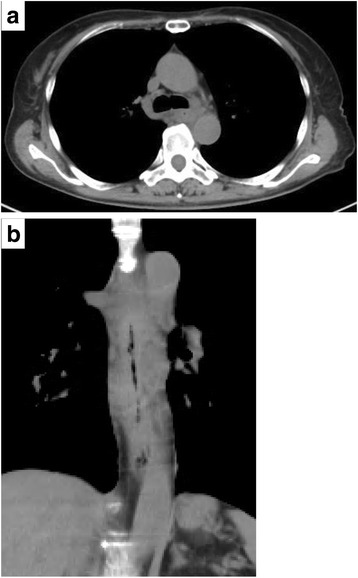
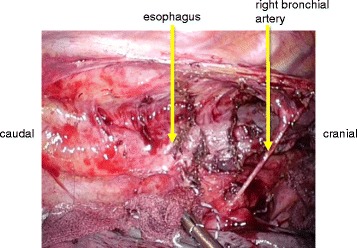
A 62-year-old woman had undergone emergency surgery for a giant ovarian tumor rupture at another hospital. A duodenal perforation occurred after surgery but improved with conservative treatment. She had undergone long-term nasogastric tube placement for 4 months because she was on a mechanical ventilator and did not receive proton pump inhibitors (PPIs). Thereafter, the patient experienced dysphagia. An esophagogastroduodenoscopy (EGD) revealed circumferential reflux esophagitis (grade D) and a stricture located 25 to 40 cm from the incisor teeth. She received medical treatment with fasting and PPIs. The second EGD revealed that the reflux esophagitis had improved somewhat, but that the esophageal stricture had worsened. Thereafter, balloon dilatation was attempted, but the stricture did not improve and she was referred to our hospital. Finally, she was diagnosed as having a benign esophageal stricture caused by reflux esophagitis. She underwent a thoracoscopic esophagectomy with gastric tube reconstruction through the antethoracic route. Her postoperative course was uneventful. Pathologically, a circumferential stricture with white scar formation and no malignant cells were observed.
We experienced a rare case requiring esophagectomy for long-segment stenosis caused by reflux esophagitis. It is suggested that the possibility of esophageal stricture needs to be kept in mind when treating GERD patients with long-term nasogastric tube placement.
大多数由胃食管反流引起的良性食管狭窄为短节段性,可通过内镜扩张治疗,但需要行食管切除术的长节段狭窄病例罕见。
一名62岁女性在另一家医院因巨大卵巢肿瘤破裂接受了急诊手术。术后发生十二指肠穿孔,但经保守治疗后好转。由于她使用机械通气且未接受质子泵抑制剂(PPI),因此长期留置鼻胃管4个月。此后,患者出现吞咽困难。食管胃十二指肠镜检查(EGD)显示为环周性反流性食管炎(D级),狭窄位于距门齿25至40厘米处。她接受了禁食和PPI药物治疗。第二次EGD显示反流性食管炎有所改善,但食管狭窄加重。此后,尝试进行球囊扩张,但狭窄未改善,遂转诊至我院。最终,她被诊断为反流性食管炎所致良性食管狭窄。她接受了胸腔镜食管切除术,并通过胸前途径行胃管重建。术后恢复顺利。病理检查显示为环周性狭窄,有白色瘢痕形成,未观察到恶性细胞。
我们遇到了一例罕见的因反流性食管炎导致长节段狭窄而需要行食管切除术的病例。提示在对长期留置鼻胃管的胃食管反流病患者进行治疗时,需要考虑食管狭窄的可能性。