Department of Obstetrics, Women and Children's Hospital of Chongqing Medical University.
Joint International Research Laboratory of Reproduction & Development, Chongqing Medical University, Yuzhong District of Chongqing.
J Hypertens. 2024 Jan 1;42(1):143-152. doi: 10.1097/HJH.0000000000003577. Epub 2023 Sep 21.
Intrahepatic cholestasis of pregnancy (ICP) is a special liver disease during pregnancy, characterized by abnormal bile acid metabolism. However, there is no consensus on how to group women with ICP based on the time of diagnosis worldwide. This study aimed to adopt a new grouping model of women with ICP, and the time from diagnosis to delivery was defined as the monitoring period.
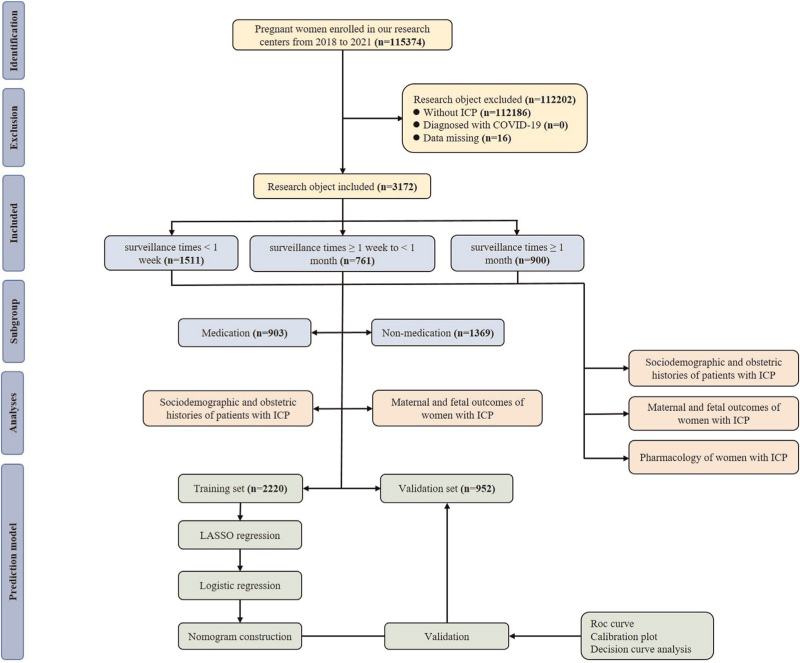
This retrospective real-world data study was conducted across multiple centers and included 3172 women with ICP. The study first evaluated the significant difference in medication and nonmedication during different monitoring times. The least absolute shrinkage and selection operator (LASSO) model was then used to screen nine risk factors based on the predictors. The model's discrimination, clinical usefulness, and calibration were assessed using the area under the receiver operating characteristic (ROC) curve, decision curve, and calibration analysis.
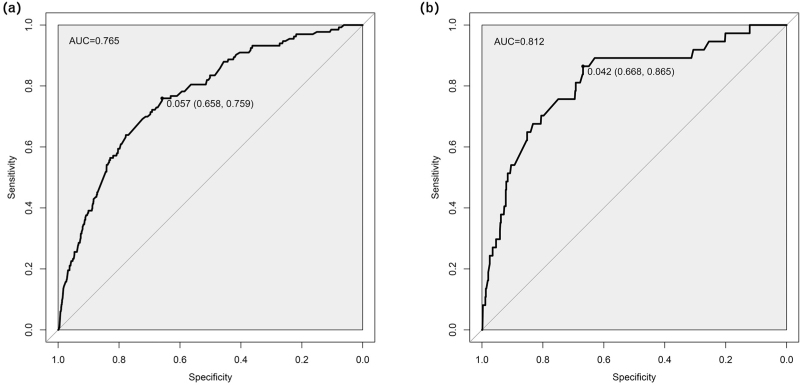
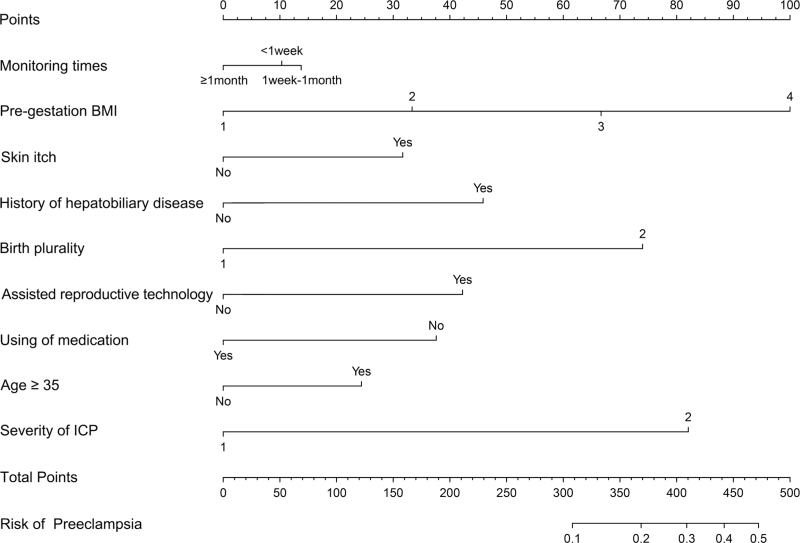
The incidence of preeclampsia risk in ICP patients without drug intervention increased with the extension of the monitoring period. However, the risk of preeclampsia decreased in ICP patients treated with ursodeoxycholic acid. A predictive nomogram and risk score model was developed based on nine risk factors. The area under the ROC curve of the nomogram was 0.765 [95% confidence interval (CI): 0.724-0.807] and 0.812 (95% CI: 0.736-0.889) for the validation cohort.
This study found that a longer ICP monitoring period could lead to adverse pregnancy outcomes in the absence of drug intervention, especially preeclampsia. A predictive nomogram and risk score model was developed to better manage ICP patients, maintain pregnancy to term delivery, and minimize the risk of severe adverse maternal and fetal outcomes.
妊娠肝内胆汁淤积症(ICP)是一种妊娠期特有的肝脏疾病,其特征为胆汁酸代谢异常。然而,目前全球范围内对于如何根据诊断时间对 ICP 患者进行分组尚未达成共识。本研究旨在采用一种新的 ICP 患者分组模型,将从诊断到分娩的时间定义为监测期。
本回顾性真实世界研究在多个中心开展,共纳入 3172 例 ICP 患者。首先评估不同监测时间点药物和非药物治疗的差异。然后,使用最小绝对收缩和选择算子(LASSO)模型基于预测因素筛选 9 个风险因素。采用受试者工作特征(ROC)曲线下面积、决策曲线和校准分析评估模型的判别力、临床实用性和校准。
未接受药物干预的 ICP 患者的子痫前期风险随监测期的延长而增加。然而,熊去氧胆酸治疗的 ICP 患者的子痫前期风险降低。基于 9 个风险因素建立了预测列线图和风险评分模型。列线图的 ROC 曲线下面积在验证队列中为 0.765(95%CI:0.724-0.807)和 0.812(95%CI:0.736-0.889)。
本研究发现,在没有药物干预的情况下,较长的 ICP 监测期可能导致不良妊娠结局,尤其是子痫前期。建立了预测列线图和风险评分模型,以更好地管理 ICP 患者,维持妊娠至足月分娩,并最大程度降低母婴严重不良结局的风险。