Department of Anesthesiology, Washington University School of Medicine in St Louis, St Louis, Missouri.
Department of Anesthesiology, University of Nebraska Medical Center, Omaha.
JAMA Netw Open. 2023 Sep 5;6(9):e2332517. doi: 10.1001/jamanetworkopen.2023.32517.
Telemedicine for clinical decision support has been adopted in many health care settings, but its utility in improving intraoperative care has not been assessed.
To pilot the implementation of a real-time intraoperative telemedicine decision support program and evaluate whether it reduces postoperative hypothermia and hyperglycemia as well as other quality of care measures.
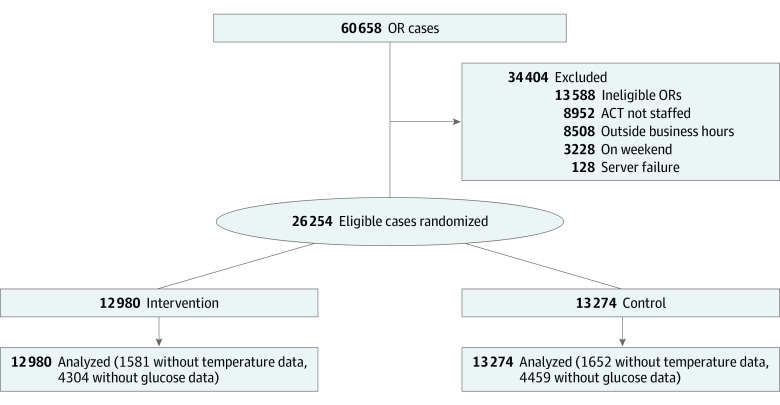
DESIGN, SETTING, AND PARTICIPANTS: This single-center pilot randomized clinical trial (Anesthesiology Control Tower-Feedback Alerts to Supplement Treatments [ACTFAST-3]) was conducted from April 3, 2017, to June 30, 2019, at a large academic medical center in the US. A total of 26 254 adult surgical patients were randomized to receive either usual intraoperative care (control group; n = 12 980) or usual care augmented by telemedicine decision support (intervention group; n = 13 274). Data were initially analyzed from April 22 to May 19, 2021, with updates in November 2022 and February 2023.
Patients received either usual care (medical direction from the anesthesia care team) or intraoperative anesthesia care monitored and augmented by decision support from the Anesthesiology Control Tower (ACT), a real-time, live telemedicine intervention. The ACT incorporated remote monitoring of operating rooms by a team of anesthesia clinicians with customized analysis software. The ACT reviewed alerts and electronic health record data to inform recommendations to operating room clinicians.
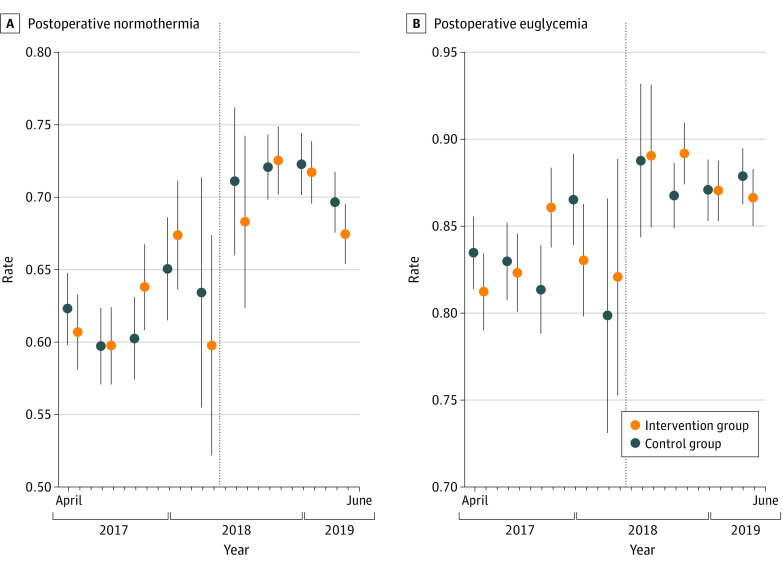
The primary outcomes were avoidance of postoperative hypothermia (defined as the proportion of patients with a final recorded intraoperative core temperature >36 °C) and hyperglycemia (defined as the proportion of patients with diabetes who had a blood glucose level ≤180 mg/dL on arrival to the postanesthesia recovery area). Secondary outcomes included intraoperative hypotension, temperature monitoring, timely antibiotic redosing, intraoperative glucose evaluation and management, neuromuscular blockade documentation, ventilator management, and volatile anesthetic overuse.
Among 26 254 participants, 13 393 (51.0%) were female and 20 169 (76.8%) were White, with a median (IQR) age of 60 (47-69) years. There was no treatment effect on avoidance of hyperglycemia (7445 of 8676 patients [85.8%] in the intervention group vs 7559 of 8815 [85.8%] in the control group; rate ratio [RR], 1.00; 95% CI, 0.99-1.01) or hypothermia (7602 of 11 447 patients [66.4%] in the intervention group vs 7783 of 11 672 [66.7.%] in the control group; RR, 1.00; 95% CI, 0.97-1.02). Intraoperative glucose measurement was more common among patients with diabetes in the intervention group (RR, 1.07; 95% CI, 1.01-1.15), but other secondary outcomes were not significantly different.
In this randomized clinical trial, anesthesia care quality measures did not differ between groups, with high confidence in the findings. These results suggest that the intervention did not affect the targeted care practices. Further streamlining of clinical decision support and workflows may help the intraoperative telemedicine program achieve improvement in targeted clinical measures.
ClinicalTrials.gov Identifier: NCT02830126.
远程医疗在临床决策支持方面已在许多医疗保健环境中得到采用,但它在改善术中护理方面的效用尚未得到评估。
试点实施实时术中远程医疗决策支持计划,并评估其是否能降低术后低体温和高血糖以及其他护理质量措施。
设计、地点和参与者:这是一项在美国一家大型学术医疗中心进行的单中心先导随机临床试验(麻醉学控制塔-反馈警报以补充治疗[ACTFAST-3])。从 2017 年 4 月 3 日至 2019 年 6 月 30 日,共有 26254 名成年手术患者被随机分配接受常规术中护理(对照组;n=12980)或常规护理加远程医疗决策支持(干预组;n=13274)。最初的数据分析于 2021 年 4 月 22 日至 5 月 19 日进行,并于 2022 年 11 月和 2023 年 2 月进行了更新。
患者接受常规护理(麻醉护理团队提供医疗指导)或接受麻醉学控制塔(ACT)的术中麻醉护理监测和增强,这是一种实时的、现场远程医疗干预措施。ACT 采用了由麻醉临床医生组成的团队对手术室进行远程监测,并结合了定制的分析软件。ACT 审查警报和电子健康记录数据,为手术室临床医生提供建议。
主要结果是避免术后低体温(定义为最后记录的术中核心体温>36°C 的患者比例)和高血糖(定义为糖尿病患者到达麻醉恢复区时血糖水平≤180mg/dL 的患者比例)。次要结果包括术中低血压、体温监测、及时抗生素重新给药、术中血糖评估和管理、神经肌肉阻滞文件记录、呼吸机管理和挥发性麻醉剂过度使用。
在 26254 名参与者中,13393 名(51.0%)为女性,20169 名(76.8%)为白人,中位(IQR)年龄为 60(47-69)岁。在避免高血糖(干预组 8676 例患者中有 7445 例[85.8%],对照组 8815 例患者中有 7559 例[85.8%];率比[RR],1.00;95%CI,0.99-1.01)或低体温(干预组 11447 例患者中有 7602 例[66.4%],对照组 11672 例患者中有 7783 例[66.7%];RR,1.00;95%CI,0.97-1.02)方面,两组均无治疗效果。在糖尿病患者中,术中血糖测量更为常见(RR,1.07;95%CI,1.01-1.15),但其他次要结果没有显著差异。
在这项随机临床试验中,两组之间的麻醉护理质量措施没有差异,对研究结果有高度信心。这些结果表明,该干预措施并未影响目标护理实践。进一步简化临床决策支持和工作流程可能有助于该术中远程医疗计划在目标临床措施方面取得改善。
ClinicalTrials.gov 标识符:NCT02830126。