Department of Population Health, NYU Grossman School of Medicine, New York, New York.
Division of Healthcare Delivery Science, Department of Population Health, NYU School of Medicine, New York, New York.
JAMA Health Forum. 2023 Sep 1;4(9):e233197. doi: 10.1001/jamahealthforum.2023.3197.
Medicaid patients with mental illness comprise one of the most high-need and complex patient populations. Value-based reforms aim to improve care, but their efficacy in the Medicaid program is unclear.
To investigate if New York state's Medicaid value-based payment reform was associated with improved utilization patterns for patients with mental illness.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study used a difference-in-differences analysis to compare changes in utilization between Medicaid beneficiaries whose outpatient practices participated in value-based payment reform and beneficiaries whose practices did not participate from before (July 1, 2013-June 30, 2015) to after reform (July 1, 2015-June 30, 2019). Participants were Medicaid beneficiaries in New York state aged 18 to 64 years with major depression disorder, bipolar disorder, and/or schizophrenia. Data analysis was performed from April 2021 to July 2023.
Beneficiaries were exposed to value-based payment reforms if their attributed outpatient practice participated in value-based payment reform at baseline (July 1, 2015).
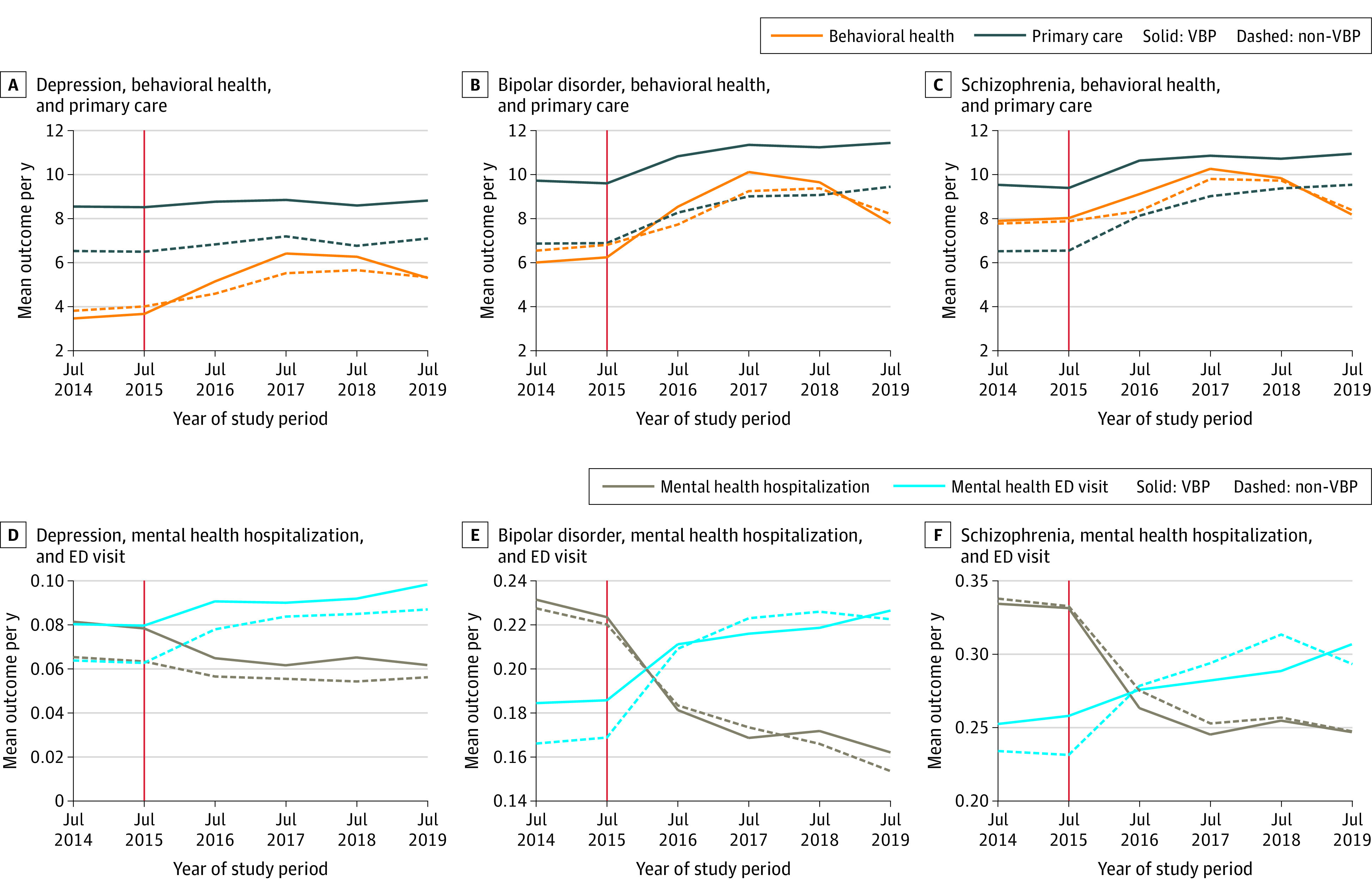
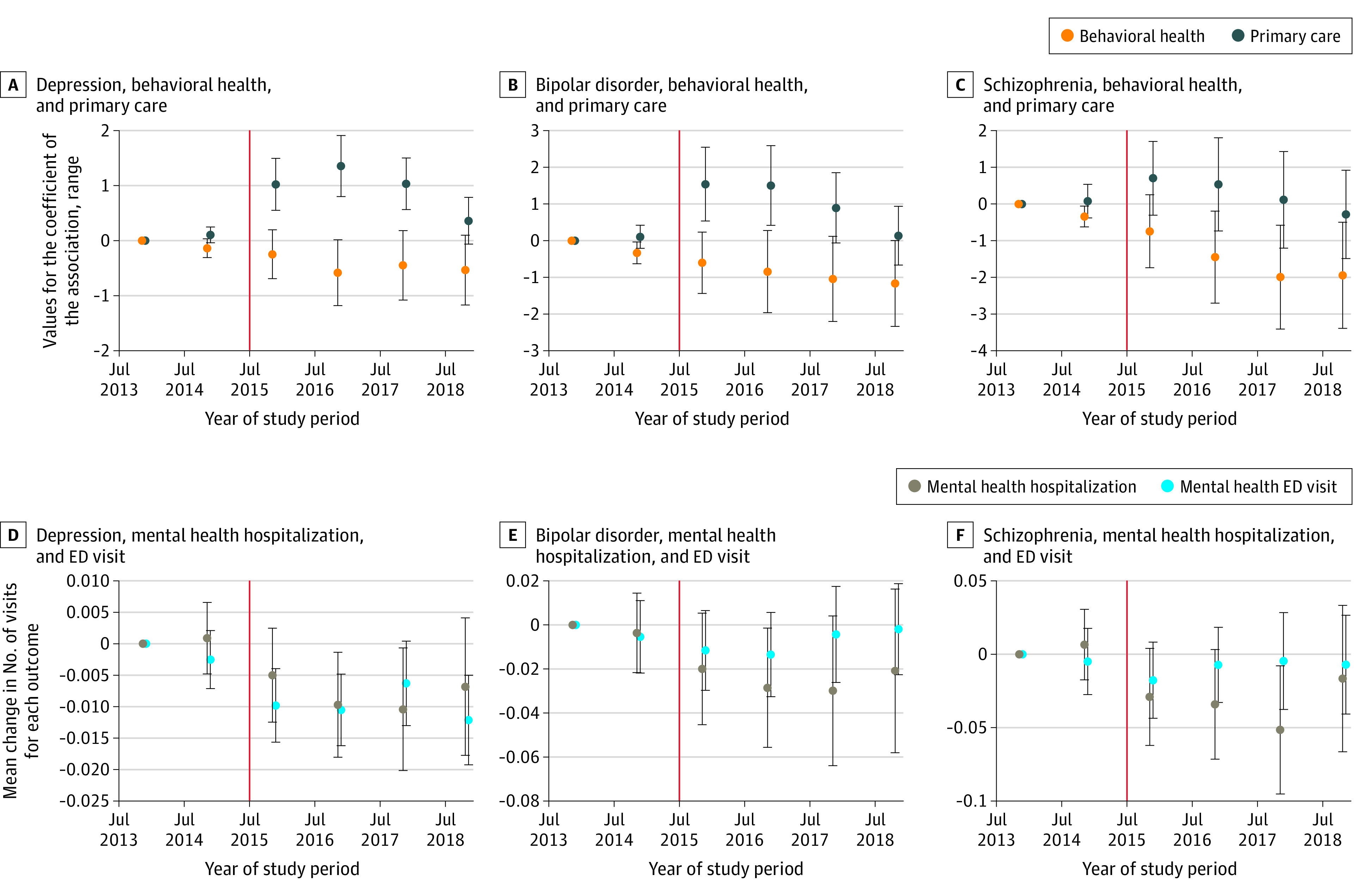
Primary outcomes were the number of outpatient primary care visits and the number of behavioral health visits per year. Secondary outcomes were the number of mental health emergency department visits and hospitalizations per year.
The analytic population comprised 306 290 individuals with depression (67.4% female; mean [SD] age, 38.6 [11.9] years), 85 105 patients with bipolar disorder (59.6% female; mean [SD] age, 38.0 [11.6] years), and 71 299 patients with schizophrenia (45.1% female; mean [SD] age, 40.3 [12.2] years). After adjustment, analyses estimated a statistically significant, positive association between value-based payments and behavioral health visits for patients with depression (0.91 visits; 95% CI, 0.51-1.30) and bipolar disorder (1.01 visits; 95% CI, 0.22-1.79). There was no statistically significant changes to primary care visits for patients with depression and bipolar disorder, but value-based payments were associated with reductions in primary care visits for patients with schizophrenia (-1.31 visits; 95% CI, -2.51 to -0.12). In every diagnostic population, value-based payment was associated with significant reductions in mental health emergency department visits (population with depression: -0.01 visits [95% CI, -0.02 to -0.002]; population with bipolar disorder: -0.02 visits [95% CI, -0.05 to -0.001]; population with schizophrenia: -0.04 visits [95% CI, -0.07 to -0.01]).
In this cohort study, Medicaid value-based payment reform was statistically significantly associated with an increase in behavioral health visits and a reduction in mental health emergency department visits for patients with mental illness. Medicaid value-based payment may be effective at altering health care utilization in patients with mental illness.
患有精神疾病的医疗补助患者是需求最高和最复杂的患者群体之一。基于价值的改革旨在改善护理,但它们在医疗补助计划中的效果尚不清楚。
调查纽约州的医疗补助基于价值的支付改革是否与精神疾病患者的利用模式改善相关。
设计、设置和参与者:这项回顾性队列研究使用差异中的差异分析,比较了在门诊实践参与基于价值的支付改革的医疗补助受益人和未参与实践的受益人(2013 年 7 月 1 日至 2015 年 6 月 30 日)在改革后(2015 年 7 月 1 日至 2019 年 6 月 30 日)的利用变化。参与者是纽约州年龄在 18 至 64 岁之间的患有重度抑郁症、双相情感障碍和/或精神分裂症的医疗补助受益人。数据分析于 2021 年 4 月至 2023 年 7 月进行。
如果受益人的归因门诊实践在基线时(2015 年 7 月 1 日)参与基于价值的支付改革,则他们将面临基于价值的支付改革。
主要结果是每年的门诊初级保健就诊次数和行为健康就诊次数。次要结果是每年的心理健康急诊就诊次数和住院次数。
分析人群包括 306290 名患有抑郁症的个体(67.4%为女性;平均[SD]年龄,38.6[11.9]岁)、85105 名患有双相情感障碍的患者(59.6%为女性;平均[SD]年龄,38.0[11.6]岁)和 71299 名患有精神分裂症的患者(45.1%为女性;平均[SD]年龄,40.3[12.2]岁)。调整后分析估计,基于价值的支付与抑郁症患者(0.91 次就诊;95%CI,0.51-1.30)和双相情感障碍患者(1.01 次就诊;95%CI,0.22-1.79)的行为健康就诊之间存在统计学上显著的正相关。抑郁症和双相情感障碍患者的初级保健就诊次数没有统计学上的显著变化,但基于价值的支付与精神分裂症患者的初级保健就诊次数减少有关(-1.31 次就诊;95%CI,-2.51 至-0.12)。在每个诊断人群中,基于价值的支付与心理健康急诊就诊次数的显著减少相关(抑郁症人群:-0.01 次就诊[95%CI,-0.02 至-0.002];双相情感障碍人群:-0.02 次就诊[95%CI,-0.05 至-0.001];精神分裂症人群:-0.04 次就诊[95%CI,-0.07 至-0.01])。
在这项队列研究中,医疗补助基于价值的支付改革与精神疾病患者的行为健康就诊次数增加和心理健康急诊就诊次数减少有统计学上的显著关联。基于价值的医疗补助支付可能在改变精神疾病患者的医疗保健利用方面是有效的。