Caiati Carlo, Pollice Paolo, Iacovelli Fortunato, Sturdà Francesca, Lepera Mario Erminio
Unit of Cardiovascular Diseases, Department of Interdisciplinary Medicine, University of Bari "Aldo Moro", Bari, Italy.
Front Cardiovasc Med. 2023 Sep 8;10:1186983. doi: 10.3389/fcvm.2023.1186983. eCollection 2023.
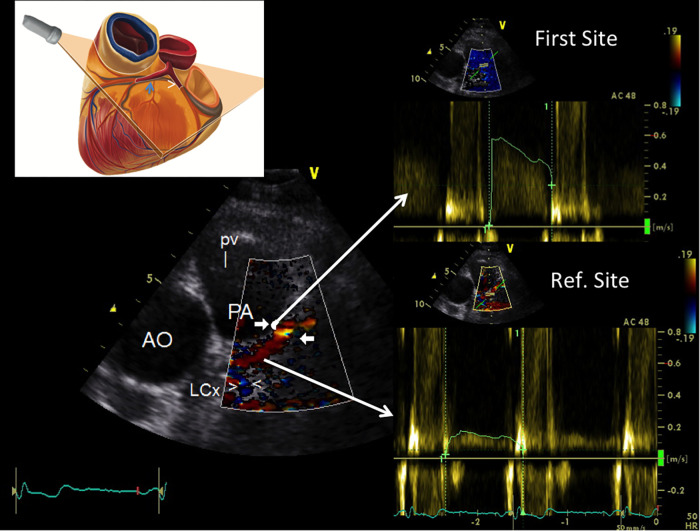
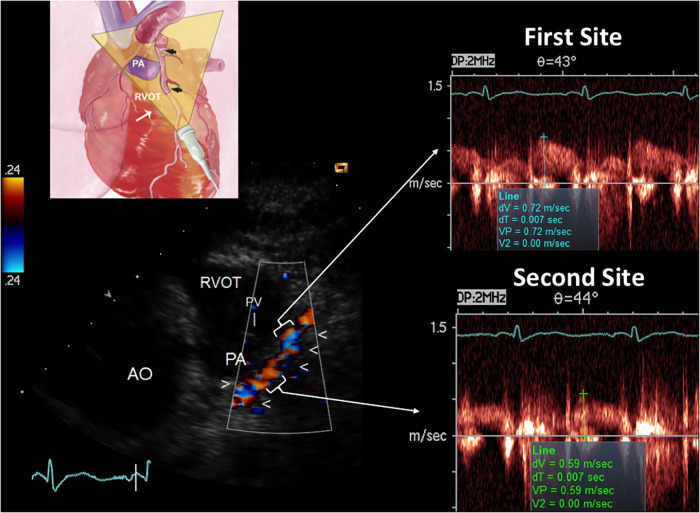
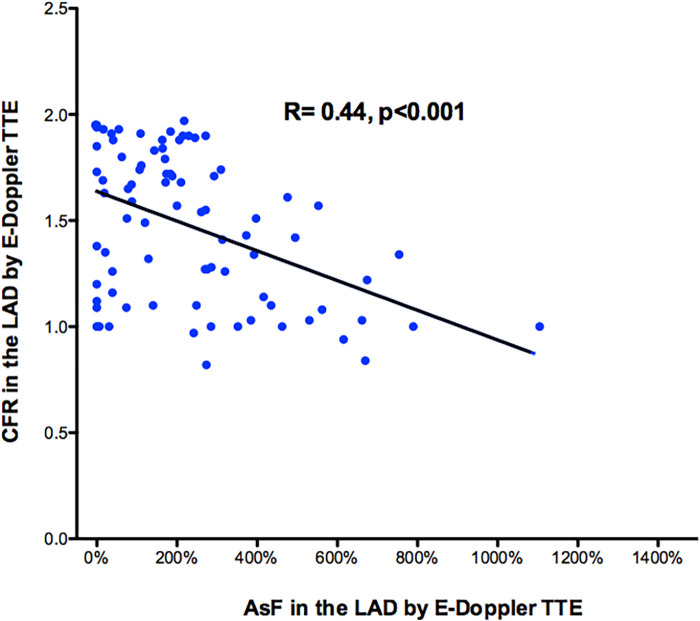
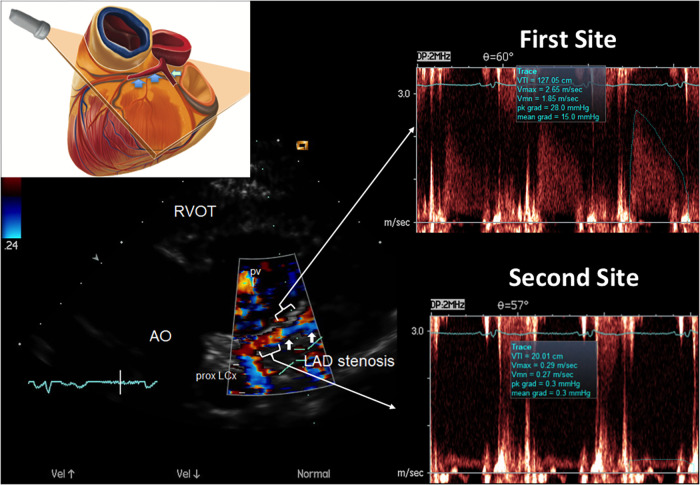
Accelerated stenotic flow (AsF) in the entire left anterior descending coronary artery (LAD), assessed by transthoracic enhanced color Doppler (E-Doppler TTE), can reveal coronary stenosis (CS) and its severity, enabling a distinction between the microcirculatory and epicardial causes of coronary flow reserve (CFR) impairment.
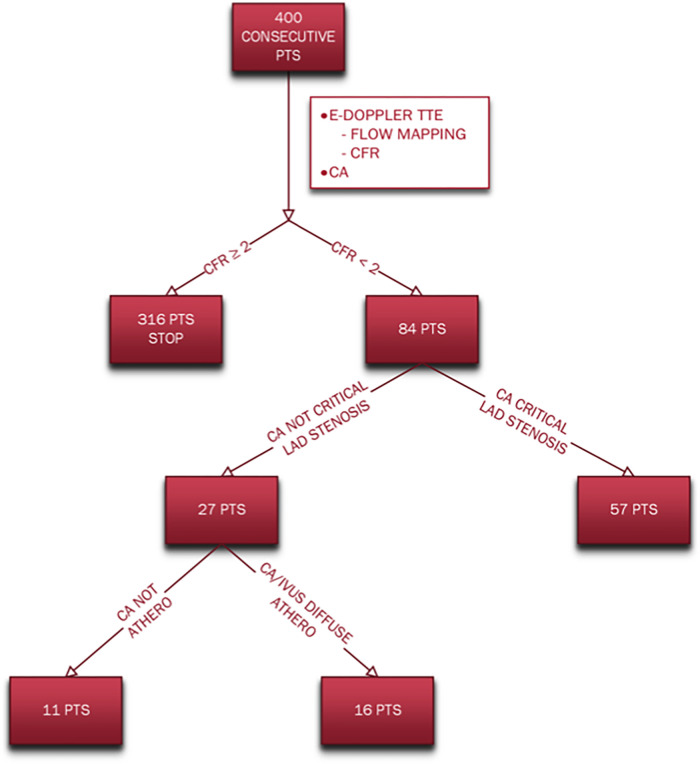
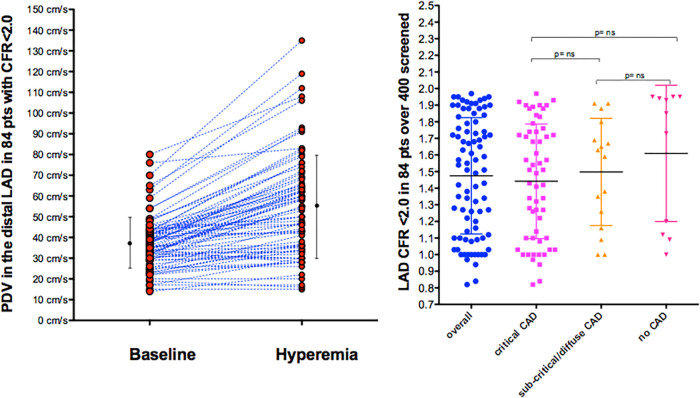
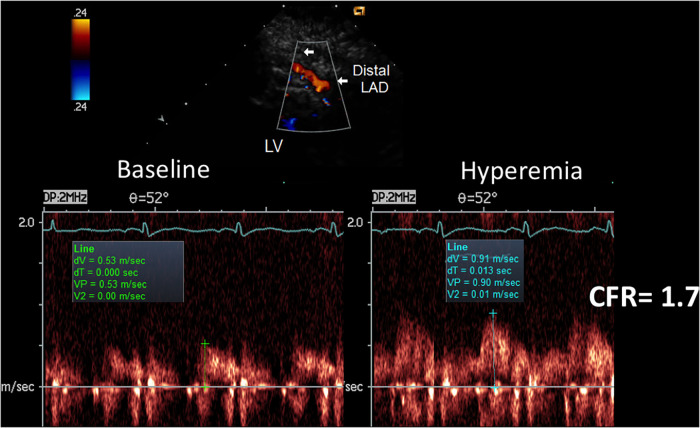
Eighty-four consecutive patients with a CFR <2.0 (1.5 ± 0.4), as assessed by E-Doppler TTE, scheduled for coronary angiography (CA) and eventually intracoronary ultrasounds (IVUS), were studied. CFR was calculated by the ratio of peak diastolic flow velocities: during i.v. adenosine (140 mcg/Kg/m) over resting; AsF was calculated as the percentage increase of localized maximal velocity in relation to a reference velocity.
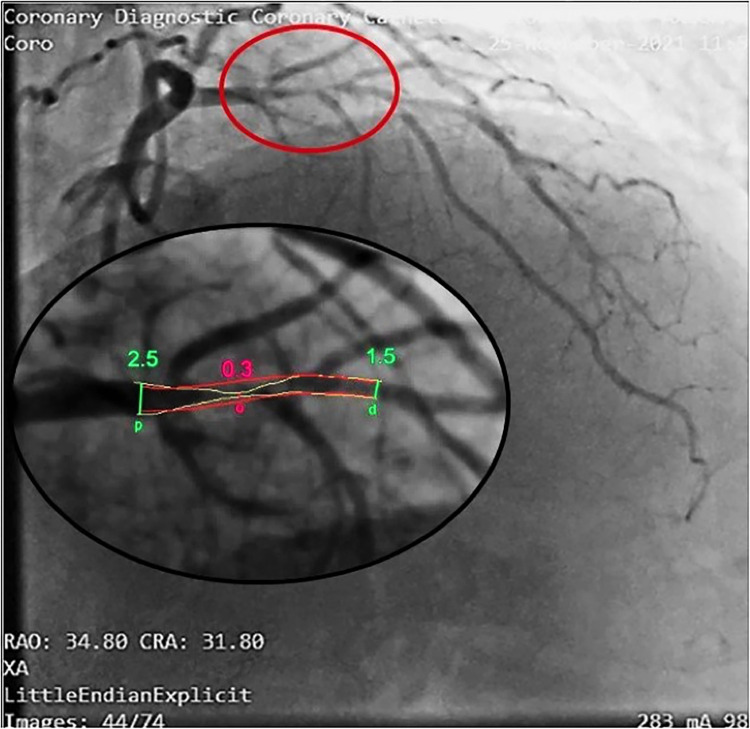
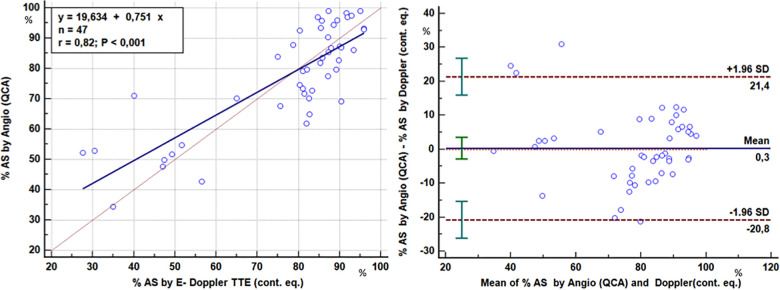
CA showed ≥50% lumen diameter narrowing of the LAD (critical CS) in 68% of patients (57/84) vs. non-critical CS in 32% (27/84). Based on the established CA/IVUS criteria, the non-critical CS subgroup was further subdivided into 2 groups: subcritical/diffuse [16/27 pts (57%)] and no atherosclerosis [11/27 pts (43%)]. CFR was similar in the three groups: 1.4 ± 0.3 in critical CS, 1.5 ± 0.4 in subcritical/diffuse CS, and 1.6 ± 0.4 in no atherosclerosis ( = ns). Overall, at least one segment of accelerated stenotic flow in the LAD was found in 73 patients (87%), while in 11 (13%) it was not. The AsF was very predictive of coronary segmental narrowing in both angio subgroups of atherosclerosis but as expected with the usage of different cutoffs. On the basis of the ROC curve, the optimal cutoff was 109% and 16% AsF % increment to successfully distinguish critical from non-critical CS (area under the curve [AUC] = 0.99, < 0.001) and diffuse/subcritical from no CS (AUC = 0.91%, < 0.001). Sensitivity and specificity were 96% and 100% and 82% and 100%, respectively.
E-Doppler TTE is highly feasible and reliable in detecting the CS of any grade of severity, distinguishing epicardial athero from microvascular causes of a severe CFR reduction.
经胸增强彩色多普勒(E-Doppler TTE)评估的整个左前降支冠状动脉(LAD)中的加速狭窄血流(AsF),可揭示冠状动脉狭窄(CS)及其严重程度,从而能够区分冠状动脉血流储备(CFR)受损的微循环和心外膜原因。
对84例连续患者进行了研究,这些患者经E-Doppler TTE评估CFR<2.0(1.5±0.4),计划进行冠状动脉造影(CA)并最终进行血管内超声(IVUS)检查。CFR通过舒张末期峰值流速之比计算:静脉注射腺苷(140μg/Kg/m)时的流速与静息时的流速之比;AsF计算为局部最大速度相对于参考速度的增加百分比。
CA显示,68%(57/84)的患者LAD管腔直径狭窄≥50%(临界CS),32%(27/84)的患者为非临界CS。根据既定的CA/IVUS标准,非临界CS亚组进一步分为2组:亚临界/弥漫性[16/27例患者(57%)]和无动脉粥样硬化[11/27例患者(43%)]。三组的CFR相似:临界CS组为1.4±0.3,亚临界/弥漫性CS组为1.5±0.4,无动脉粥样硬化组为1.6±0.4(P=无显著性差异)。总体而言,73例患者(87%)在LAD中发现至少一段加速狭窄血流,而11例患者(13%)未发现。AsF在动脉粥样硬化的两个血管造影亚组中对冠状动脉节段性狭窄都具有很高的预测性,但正如预期的那样,使用了不同的截断值。根据ROC曲线,最佳截断值分别为109%和16%的AsF%增量,以成功区分临界与非临界CS(曲线下面积[AUC]=0.99,P<0.001)以及弥漫性/亚临界与无CS(AUC=0.91%,P<0.001)。敏感性和特异性分别为96%和100%以及82%和100%。
E-Doppler TTE在检测任何严重程度的CS方面高度可行且可靠,能够区分心外膜动脉粥样硬化与严重CFR降低的微血管原因。