Caiati Carlo, Pollice Paolo, Lepera Mario Erminio
Institute of Cardiovascular Disease, Department of Interdisciplinary Medicine, University of Bari "Aldo Moro", 70124 Bari, Italy.
Diagnostics (Basel). 2023 Feb 10;13(4):670. doi: 10.3390/diagnostics13040670.
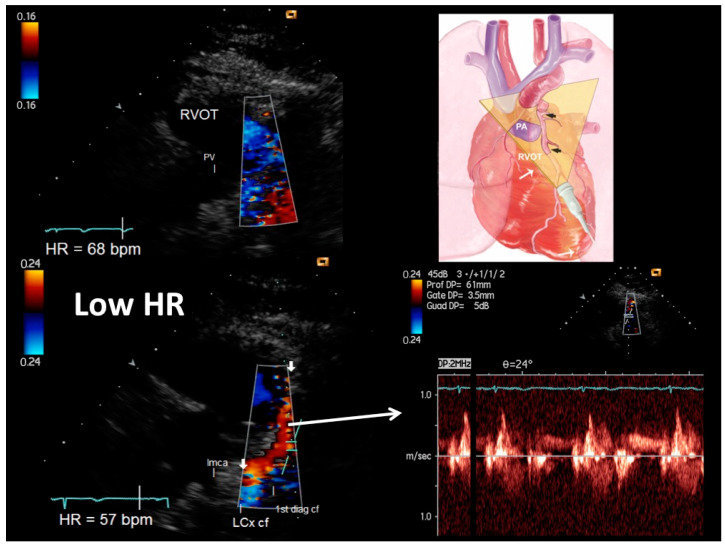
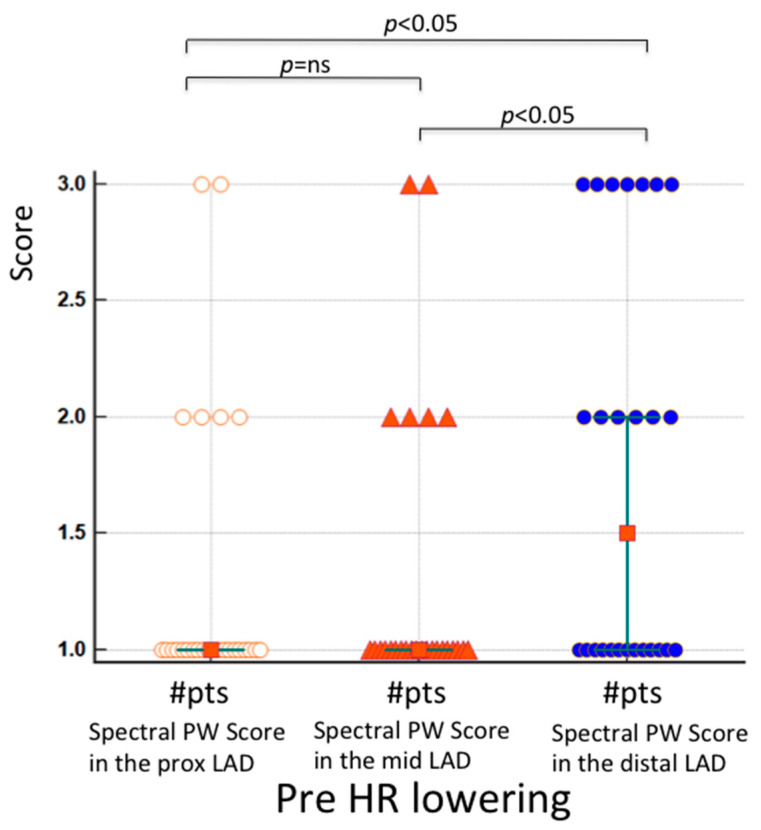
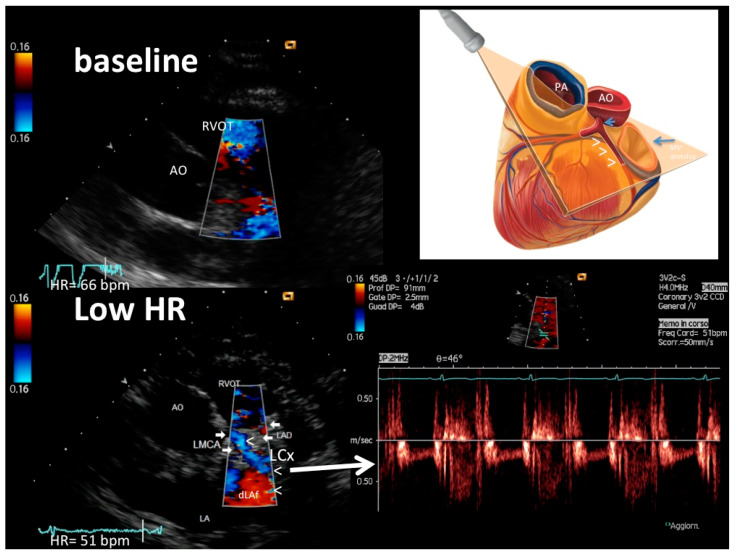
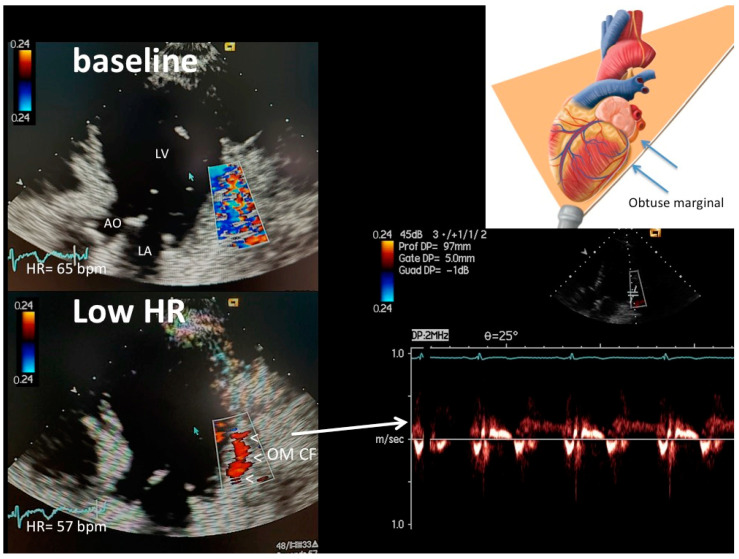
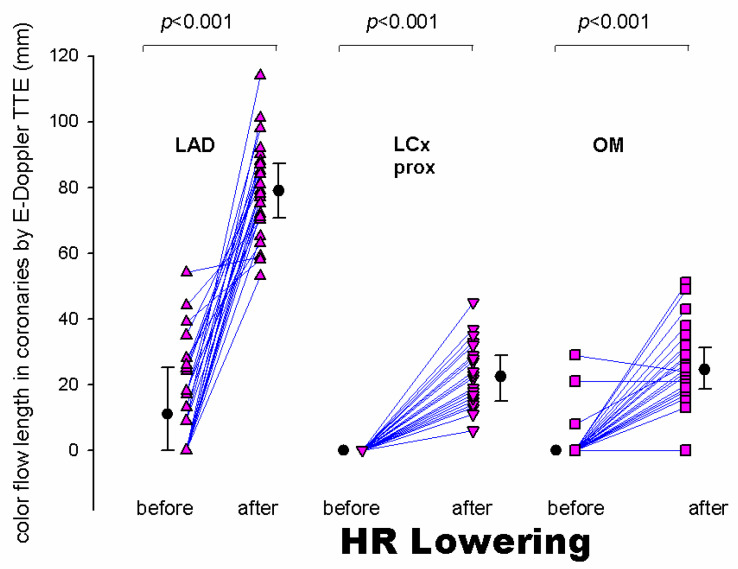
: Coronary blood flow Doppler recording by Transthoracic Doppler in convergent mode (E-Doppler TTE) might be further improved by lowering heart rate (HRL) down to <60 bpm, since low HR < 60 b/m causes a disproportional lengthening of the diastole, so the coronaries are still for a longer time, very much improving the Doppler signal/noise ratio. : A group of 26 patients underwent E-Doppler TTE before and after HR lowering in four branches of the coronary tree, namely, the left main (LMCA); left anterior descending (LAD), subdivided into three segments: proximal, mid and distal; proximal left circumflex (LCx); and obtuse marginal (OM). Color and PW coronary Doppler signal was judged by two expert observers as undetectable (SCORE 1), weak or with clutter artifacts (SCORE 2), or well delineated (SCORE 3). In addition, local accelerated stenotic flow (AsF) was measured in the LAD before and after HRL. : Beta-blockers significantly decreased the mean HR from 76 ± 5 to 57 ± 6 bpm ( < 0.001). Before HRL, the Doppler quality was very poor in the proximal and mid-LAD segments (median score value = 1 in both), while in the distal LAD, it was significantly better but still suboptimal (median score value = 1.5, = 0.009 vs. proximal and mid-LAD score). After HRL, blood flow Doppler recording in the three LAD segments was strikingly improved (median score value = 3, 3 and 3, = ns), so the effect of HRL was more efficacious in the two more proximal LAD segments. In 10 patients undergoing coronary angiography (CA), no AsF as expression of transtenotic velocity was detected at baseline. After HRL, thanks to the better quality and length of color flow, ASF was detected in five patients while in five others, it was not in perfect agreement with CA (Spearman correlation coefficient = 1, < 0.01). The color flow in the proximal LCx and OM was extremely poor at baseline (color flow length 0 and 0, median (interquartile range) mm, respectively) and improved considerably after HRL (color flow length 23 [13.5] and 25 [12.0] mm, respectively, < 0.001). : HRL greatly improved the success rate of blood flow Doppler recording in coronaries, not only in the LAD, but also in the LCx. Therefore, AsF for stenosis detection and coronary flow reserve assessment can have wider clinical applications. However, further studies with larger samples are needed to confirm these results.
经胸多普勒在收敛模式下(E-Doppler TTE)进行冠状动脉血流多普勒记录,通过将心率(HRL)降低至<60次/分钟可能会进一步改善,因为低心率<60次/分钟会导致舒张期不成比例地延长,因此冠状动脉处于舒张期的时间更长,这极大地提高了多普勒信号/噪声比。一组26例患者在心率降低前后,对冠状动脉树的四个分支进行了E-Doppler TTE检查,这四个分支分别是左主干(LMCA);左前降支(LAD),细分为三段:近端、中段和远端;近端左旋支(LCx);钝缘支(OM)。两名专家观察者将彩色和脉冲波冠状动脉多普勒信号判定为不可检测(评分1)、微弱或有杂波伪像(评分2)或清晰可辨(评分3)。此外,在心率降低前后测量了LAD处的局部加速狭窄血流(AsF)。β受体阻滞剂使平均心率从76±5次/分钟显著降低至57±6次/分钟(<0.001)。在心率降低前,LAD近端和中段的多普勒质量非常差(两者的中位数评分值均为1),而在LAD远端,质量明显更好但仍未达到最佳(中位数评分值为1.5,与近端和中段LAD评分相比,P=0.009)。心率降低后,LAD三个节段的血流多普勒记录显著改善(中位数评分值均为3,P=无显著差异),因此心率降低对LAD近端两个节段的效果更显著。在10例行冠状动脉造影(CA)的患者中,基线时未检测到作为跨狭窄速度表达的AsF。心率降低后,由于彩色血流质量更好、长度更长,5例患者检测到了AsF,而另外5例患者检测到的结果与CA不完全一致(Spearman相关系数=1,P<0.01)。LCx近端和OM的彩色血流在基线时极差(彩色血流长度分别为0和0,中位数(四分位间距)mm),心率降低后显著改善(彩色血流长度分别为23[13.5]和25[12.0]mm,P<0.001)。心率降低极大地提高了冠状动脉血流多普勒记录的成功率,不仅在LAD,在LCx也如此。因此,用于狭窄检测和冠状动脉血流储备评估的AsF可具有更广泛的临床应用。然而,需要更大样本量的进一步研究来证实这些结果。