Praktiknjo Michael, Shawcross Debbie, Laleman Wim
Department of Medicine B, Gastroenterology, Hepatology, Endocrinology, Infectious Diseases, Universitätsklinikum Münster, Münster, Germany.
Institute of Liver Studies, Department of Inflammation Biology, School of Immunology and Microbial Sciences, Faculty of Life Sciences and Medicine, King's College London, London, UK.
Liver Int. 2025 Mar;45(3):e15749. doi: 10.1111/liv.15749. Epub 2023 Sep 27.
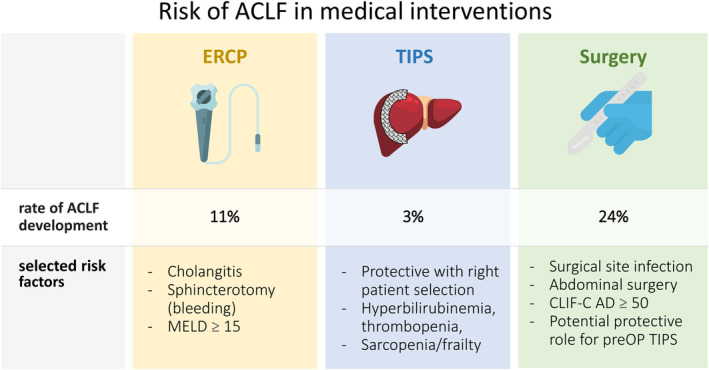
Acute-on-chronic liver failure (ACLF) is a specific, but complex and multifactorial form of acute decompensation (AD) of cirrhosis and is characterized by an extraordinary dynamic natural course, rapidly evolving organ failure and high short-term mortality. In daily clinical practice, patients with liver cirrhosis and decompensation have indications for different medical procedures such as endoscopies, interventional treatments like transjugular intrahepatic portosystemic shunt (TIPS) or even surgical procedures. In these situations, clinicians often need to balance the expected benefits of such procedures with the risks of causing acute decompensation or ACLF. This review summarizes the evidence of medical procedures and their role in precipitating or preventing ACLF and highlights the aspects to consider during patient selection.
慢加急性肝衰竭(ACLF)是肝硬化急性失代偿(AD)的一种特殊但复杂且多因素的形式,其特点是自然病程异常动态、器官功能迅速恶化以及短期死亡率高。在日常临床实践中,肝硬化失代偿患者有不同医疗程序的指征,如内镜检查、经颈静脉肝内门体分流术(TIPS)等介入治疗甚至外科手术。在这些情况下,临床医生常常需要权衡此类程序的预期益处与导致急性失代偿或ACLF的风险。本综述总结了医疗程序及其在引发或预防ACLF方面作用的证据,并强调了患者选择过程中需考虑的方面。