Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden.
Department of Psychiatry, Warneford Hospital, University of Oxford, Oxford, United Kingdom.
JAMA Psychiatry. 2024 Jan 1;81(1):25-33. doi: 10.1001/jamapsychiatry.2023.3555.
Antidepressants are increasingly prescribed to pediatric patients with unipolar depression, but little is known about the risk of treatment-emergent mania. Previous research suggests pediatric patients may be particularly vulnerable to this adverse outcome.
To estimate whether pediatric patients treated with antidepressants have an increased incidence of mania/hypomania compared with patients not treated with antidepressants and to identify patient characteristics associated with the risk of mania/hypomania.
DESIGN, SETTING, AND PARTICIPANTS: In a cohort study applying the target trial emulation framework, nationwide inpatient and outpatient care in Sweden from July 1, 2006, to December 31, 2019, was evaluated. Follow-up was conducted for 12 and 52 weeks after treatment initiation, with administrative follow-up ending December 31, 2020. Data were analyzed between May 1, 2022, and June 28, 2023. Individuals aged 4 to 17 years with a diagnosis of depression, but without a prior diagnosis of mania/hypomania, bipolar disorder, or psychosis or treatment with mood stabilizer (lithium, valproate, or carbamazepine), prescriptions were included.
The treatment group included patients who initiated any antidepressant medication within 90 days of diagnosis. The control group included patients who did not initiate antidepressants within 90 days.
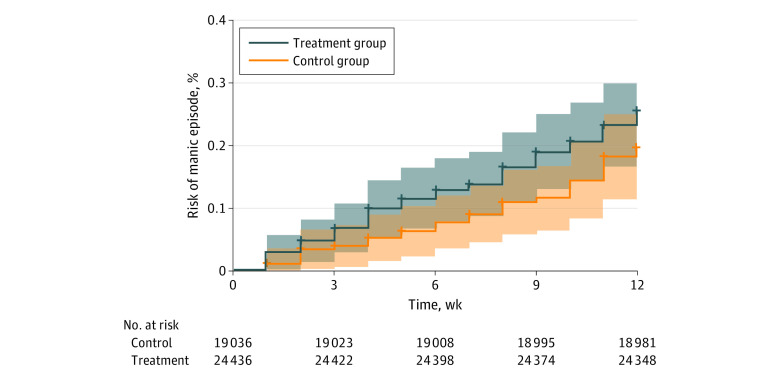
Diagnosis of mania/hypomania or initiation of mood stabilizer therapy. Incidences were estimated with Kaplan-Meier estimator, and inverse probability of treatment weighting was used to adjust for group differences at baseline.
The cohort included 43 677 patients (28 885 [66%] girls); 24 573 in the treatment group and 19 104 in the control group. The median age was 15 (IQR, 14-16) years. The outcome occurred in 96 individuals by 12 weeks and in 291 by 52 weeks. The cumulative incidence of mania was 0.26% (95% CI, 0.19%-0.33%) in the treatment group and 0.20% (95% CI, 0.13%-0.27%) in the control group at 12 weeks, with a risk difference of 0.06% (95% CI, -0.04% to 0.16%). At 52 weeks, the cumulative incidence was 0.79% (95% CI, 0.68%-0.91%) in the treatment group and 0.52% (95% CI, 0.40%-0.63%) in the control group (risk difference, 0.28%; 95% CI, 0.12%-0.44%). Hospitalizations, parental bipolar disorder, and use of antipsychotics and antiepileptics were the most important predictors of mania/hypomania by 12 weeks.
This cohort study found no evidence of treatment-emergent mania/hypomania by 12 weeks in children and adolescents. This corresponds to the time frame for antidepressants to exert their psychotropic effect. A small risk difference was found only with longer follow-up. Certain patient characteristics were associated with mania/hypomania, which warrants clinical attention.
抗抑郁药越来越多地用于治疗单相抑郁症的儿科患者,但对于治疗后出现躁狂的风险知之甚少。先前的研究表明,儿科患者可能特别容易受到这种不良后果的影响。
评估与未接受抗抑郁药治疗的患者相比,接受抗抑郁药治疗的儿科患者是否会出现更高的躁狂/轻躁狂发病率,并确定与躁狂/轻躁狂风险相关的患者特征。
设计、地点和参与者:在一项应用目标试验模拟框架的队列研究中,评估了 2006 年 7 月 1 日至 2019 年 12 月 31 日瑞典全国的住院和门诊医疗。在治疗开始后 12 周和 52 周进行随访,行政随访于 2020 年 12 月 31 日结束。数据于 2022 年 5 月 1 日至 2023 年 6 月 28 日之间进行分析。包括年龄在 4 至 17 岁之间的患有抑郁症但无躁狂/轻躁狂、双相障碍或精神病或接受情绪稳定剂(锂、丙戊酸或卡马西平)治疗史的患者。
治疗组包括在诊断后 90 天内开始任何抗抑郁药物治疗的患者。对照组包括在 90 天内未开始抗抑郁药物治疗的患者。
诊断为躁狂/轻躁狂或开始使用情绪稳定剂治疗。采用 Kaplan-Meier 估计器估计发病率,并用逆概率治疗加权法调整基线时的组间差异。
该队列包括 43677 名患者(28885 名女孩,占 66%);治疗组 24573 名,对照组 19104 名。中位年龄为 15 岁(IQR,14-16 岁)。在 12 周时,有 96 人出现了该结果,在 52 周时有 291 人出现了该结果。治疗组的躁狂累积发生率为 0.26%(95%CI,0.19%-0.33%),对照组为 0.20%(95%CI,0.13%-0.27%),差异为 0.06%(95%CI,-0.04%至 0.16%)。在 52 周时,治疗组的累积发生率为 0.79%(95%CI,0.68%-0.91%),对照组为 0.52%(95%CI,0.40%-0.63%)(差异为 0.28%;95%CI,0.12%-0.44%)。在 12 周时,住院治疗、父母的双相障碍以及使用抗精神病药和抗癫痫药是躁狂/轻躁狂的最重要预测因素。
这项队列研究发现,在儿童和青少年中,在 12 周时没有证据表明出现治疗后躁狂/轻躁狂。这与抗抑郁药发挥其精神作用的时间框架相对应。只有在更长的随访时间中才发现了很小的风险差异。某些患者特征与躁狂/轻躁狂有关,这需要临床关注。