Division of Hematology/Oncology, Northwestern University Feinberg School of Medicine, Chicago, IL.
Robert H. Lurie Comprehensive Cancer Center, Chicago, IL.
Blood Adv. 2023 Dec 12;7(23):7361-7368. doi: 10.1182/bloodadvances.2023011271.
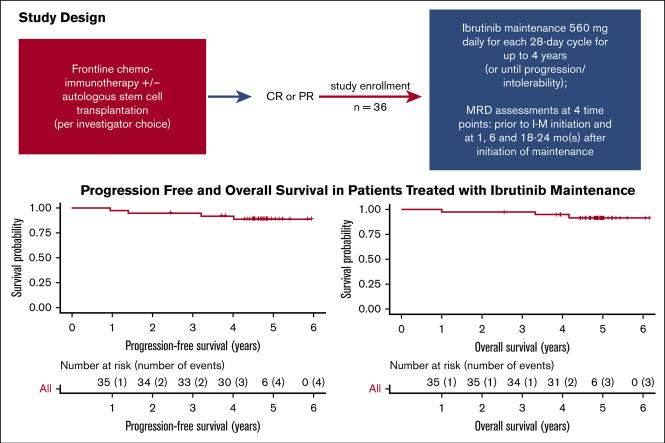
Maintenance rituximab in mantle cell lymphoma (MCL) has improved survival and supports exploration of maintenance with novel agents. We evaluated the safety and efficacy of ibrutinib maintenance (I-M) after induction in patients with treatment-naive MCL. Patients with MCL with complete response (CR) or partial response to frontline chemoimmunotherapy ± autologous stem cell transplantation (auto-SCT) received I-M 560 mg daily for up to 4 years. Primary objective was 3-year progression-free survival (PFS) rate from initiation of I-M. Minimal residual disease (MRD) assessments by next-generation sequencing (NGS) on peripheral blood were measured before I-M initiation and at 1, 6, and 18 to 24 months after initiation. Among 36 patients, the median age was 60 years (range, 46-90). For frontline treatment, 18 patients (50%) had consolidation with auto-SCT in CR1 before I-M. At median follow-up of 55.7 months, 17 patients (47%) completed full course I-M (median, 37.5 cycles; range, 2-52). The 3-year PFS and overall survival (OS) rates were 94% and 97%, respectively. With prior auto-SCT, 3-year PFS and OS rates were both 100%. The most common treatment-related adverse event with I-M was infection (n = 31; 86%), typically low grade; the most common grade 3/4 toxicities were hematologic. In 22 patients with MRD assessments, all were MRD negative after induction. Six became MRD positive on I-M, with 2 reverting to MRD-negative status with continued I-M, and all maintain radiographic CR with the exception of 1 with disease progression. I-M is feasible in MCL after frontline chemoimmunotherapy with manageable toxicities although significant. Changes in NGS-MRD were noted in limited patients during maintenance with few progression and survival events. This trial was registered at www.clinicaltrials.gov as #NCT02242097.
伊布替尼维持治疗在套细胞淋巴瘤中的应用(MCL)改善了患者的生存,为新型药物维持治疗提供了探索方向。我们评估了在初治 MCL 患者中,诱导治疗后应用伊布替尼维持治疗(I-M)的安全性和疗效。完全缓解(CR)或部分缓解(PR)患者接受一线化疗免疫治疗±自体造血干细胞移植(auto-SCT)后,每日口服伊布替尼 560mg,最长持续 4 年。主要研究终点为 I-M 起始后 3 年的无进展生存率(PFS)。在 I-M 开始前、开始后 1、6、18-24 个月,采用下一代测序(NGS)检测外周血微小残留病灶(MRD)。36 例患者的中位年龄为 60 岁(范围,46-90 岁)。18 例(50%)患者在 I-M 前已行巩固 auto-SCT 并达到 CR1。中位随访时间为 55.7 个月时,17 例(47%)患者完成了全疗程 I-M(中位 37.5 个周期;范围,2-52 个周期)。3 年 PFS 和总生存率(OS)分别为 94%和 97%。既往接受 auto-SCT 的患者,3 年 PFS 和 OS 率均为 100%。I-M 最常见的治疗相关不良事件是感染(n=31;86%),通常为低级别;最常见的 3/4 级毒性是血液学毒性。在 22 例可评估 MRD 的患者中,所有患者在诱导后均为 MRD 阴性。6 例患者在 I-M 期间转为 MRD 阳性,其中 2 例继续 I-M 后转为 MRD 阴性,除 1 例疾病进展外,所有患者均保持影像学 CR。虽然有明显毒性,但 I-M 在一线化疗免疫治疗后用于 MCL 是可行的。在维持治疗期间,少数患者的 NGS-MRD 发生了变化,进展和生存事件较少。该试验在 www.clinicaltrials.gov 注册,编号为 #NCT02242097。