Godoi Amanda, Reis Marques Isabela, Padrão Eduardo M H, Mahesh Ashwin, Hespanhol Larissa C, Riceto Loyola Júnior José Eduardo, de Souza Isabela A F, Moreira Vittoria C S, Silva Caroliny H, Miyawaki Isabele A, Oommen Christi, Gomes Cintia, Silva Ariadne C, Advani Kavita, de Sa Joao Roberto
Cardiff University School of Medicine, Neuadd Meirionnydd, Cardiff, CF144YS, UK.
Universitat Internacional de Catalunya, Barcelona, Spain.
Diabetol Metab Syndr. 2023 Sep 28;15(1):190. doi: 10.1186/s13098-023-01144-4.
Glycaemic control of Type 1 Diabetes Mellitus (T1DM) remains a challenge due to hypoglycaemic episodes and the burden of insulin self-management. Advancements have been made with the development of automated insulin delivery (AID) devices, yet, previous reviews have only assessed the use of AID over days or weeks, and potential benefits with longer time of AID use in this population remain unclear.
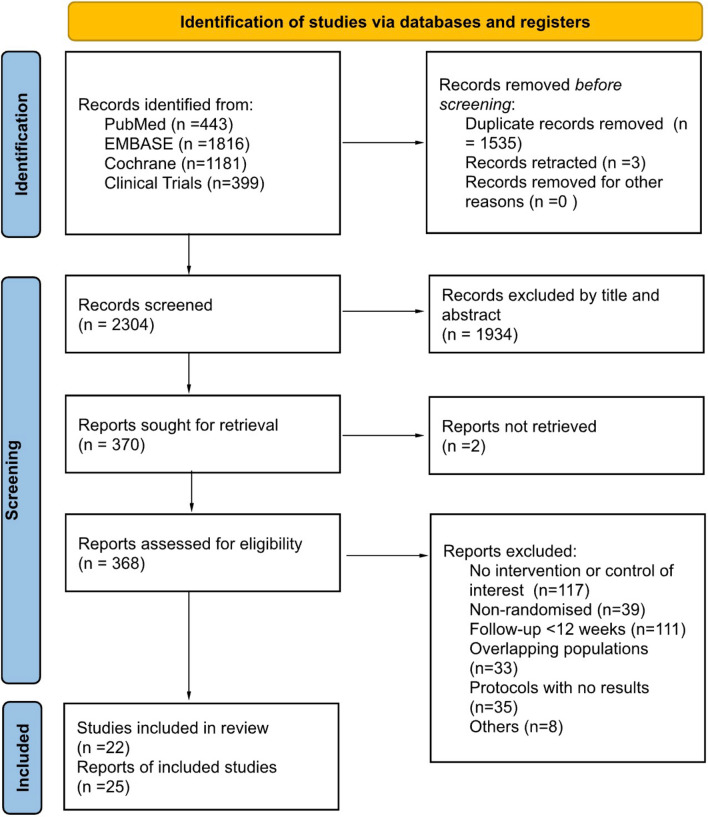
We performed a systematic review and meta-analysis of randomised controlled trials comparing AID (hybrid and fully closed-loop systems) to usual care (sensor augmented pumps, multiple daily insulin injections, continuous glucose monitoring and predictive low-glucose suspend) for adults and children with T1DM with a minimum duration of 3 months. We searched PubMed, Embase, Cochrane Central, and Clinicaltrials.gov for studies published up until April 4, 2023. Main outcomes included time in range 70-180 mg/dL as the primary outcome, and change in HbA1c (%, mmol/mol), glucose variability, and psychosocial impact (diabetes distress, treatment satisfaction and fear of hypoglycaemia) as secondary outcomes. Adverse events included diabetic ketoacidosis (DKA) and severe hypoglycaemia. Statistical analyses were conducted using mean differences and odds ratios. Sensitivity analyses were performed according to age, study duration and type of AID device. The protocol was registered in PROSPERO, CRD42022366710.
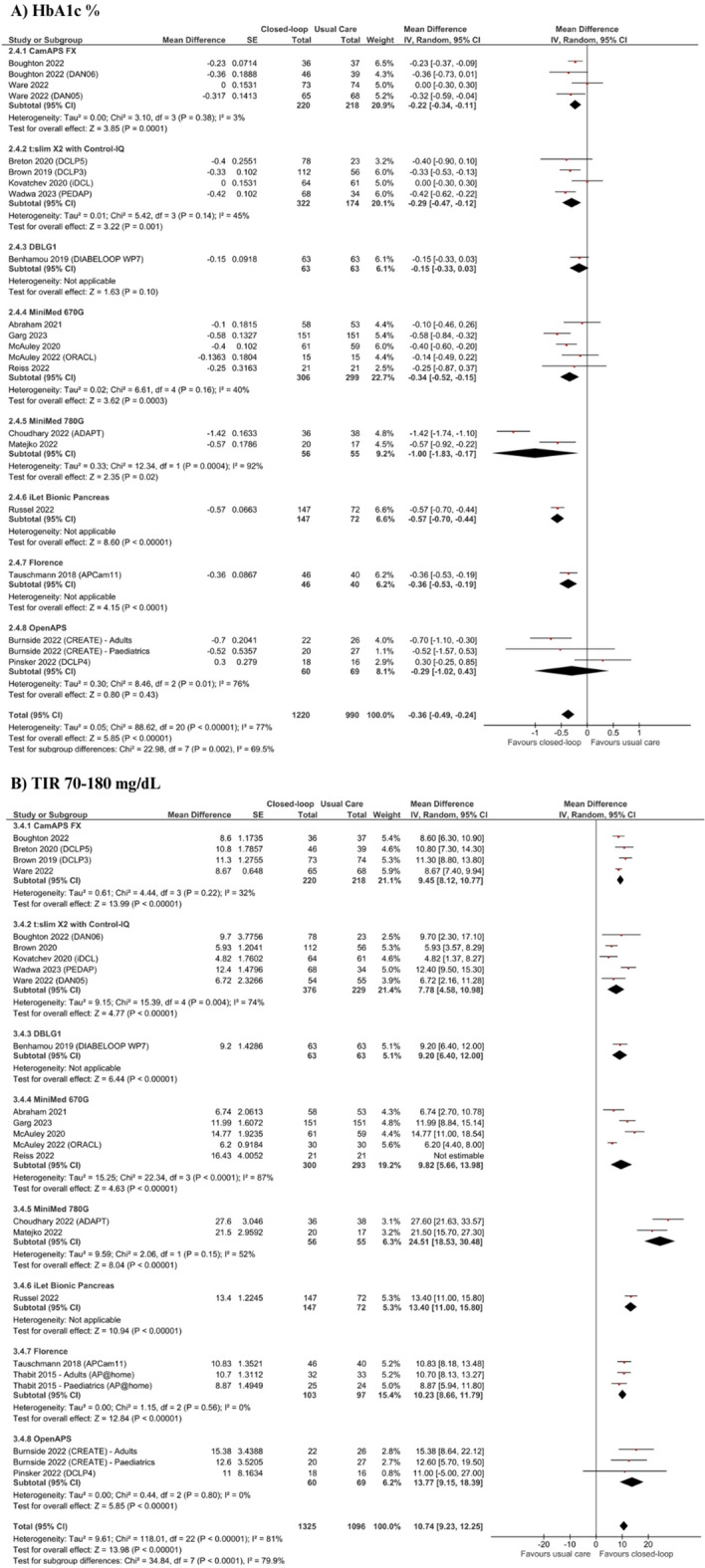
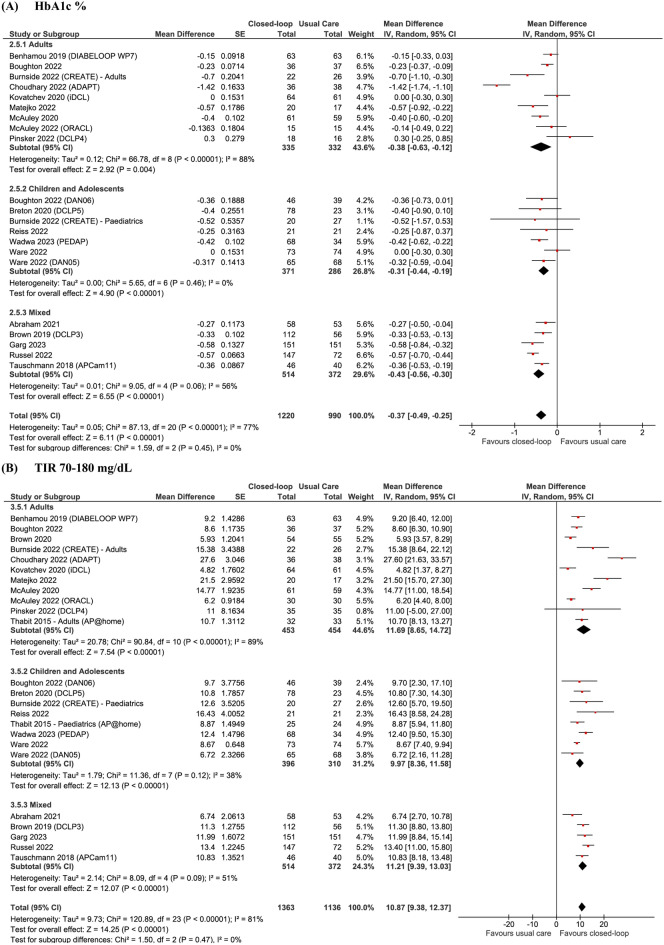
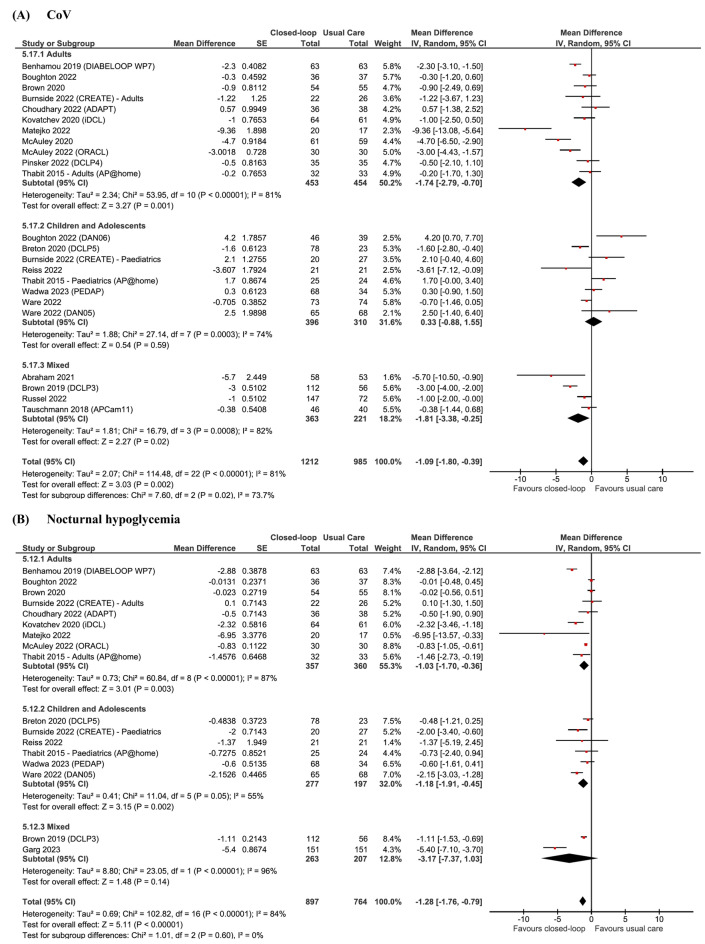
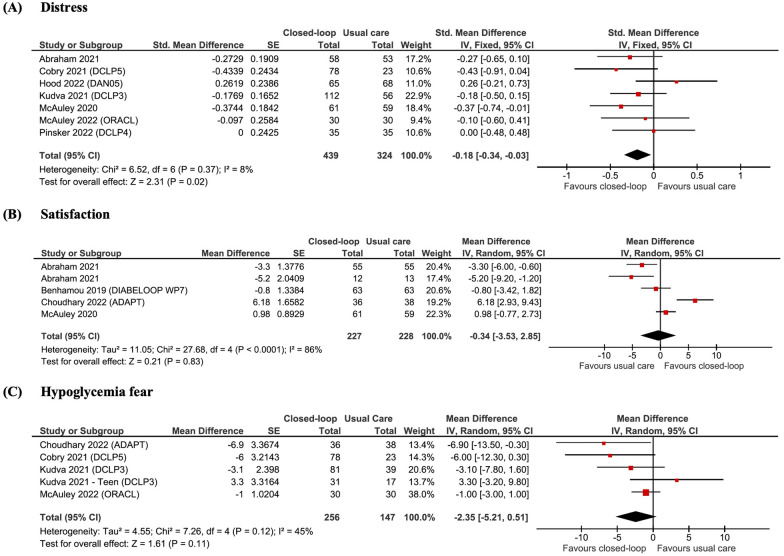
We identified 25 comparisons from 22 studies (six crossover and 16 parallel designs) including a total of 2376 participants (721 in adult studies, 621 in paediatric studies, and 1034 in combined studies) which were eligible for analysis. Use of AID devices ranged from 12 to 96 weeks. Patients using AID had 10.87% higher time in range [95% CI 9.38 to 12.37; p < 0.0001, I = 87%) and 0.37% (4.77 mmol/mol) lower HbA1c (95% CI - 0.49% (- 6.39 mmol/mol) to - 0.26 (- 3.14 mmol/mol); p < 0·0001, I = 77%]. AID systems decreased night hypoglycaemia, time in hypoglycaemia and hyperglycaemia and improved patient distress, with no increase in the risk of DKA or severe hypoglycaemia. No difference was found regarding treatment satisfaction or fear of hypoglycaemia. Among children, there was no difference in glucose variability or time spent in hypoglycaemia between the use of AID systems or usual care. In sensitivity analyses, results remained consistent with the overall analysis favouring AID.
The use of AID systems over 12 weeks, regardless of technical or clinical differences, improved glycaemic outcomes and diabetes distress without increasing the risk of adverse events in adults and children with T1DM.
由于低血糖发作以及胰岛素自我管理的负担,1型糖尿病(T1DM)的血糖控制仍然是一项挑战。随着自动胰岛素输送(AID)设备的发展,已经取得了一些进展,然而,以往的综述仅评估了AID在数天或数周内的使用情况,在该人群中使用AID更长时间的潜在益处仍不明确。
我们对随机对照试验进行了系统评价和荟萃分析,比较了AID(混合和完全闭环系统)与常规治疗(传感器增强型泵、每日多次胰岛素注射、持续葡萄糖监测和预测性低血糖暂停)对T1DM成人和儿童的疗效,试验持续时间至少为3个月。我们检索了截至2023年4月4日在PubMed、Embase、Cochrane Central和Clinicaltrials.gov上发表的研究。主要结局包括血糖在70-180mg/dL范围内的时间作为主要结局,糖化血红蛋白(HbA1c)的变化(%,mmol/mol)、血糖变异性和心理社会影响(糖尿病困扰、治疗满意度和低血糖恐惧)作为次要结局。不良事件包括糖尿病酮症酸中毒(DKA)和严重低血糖。使用均数差值和比值比进行统计分析。根据年龄、研究持续时间和AID设备类型进行敏感性分析。该方案已在PROSPERO注册,注册号为CRD42022366710。
我们从22项研究(6项交叉设计和16项平行设计)中确定了25项比较,共2376名参与者(成人研究721名,儿科研究621名,综合研究1034名)符合分析条件。AID设备的使用时间为12至96周。使用AID的患者血糖在目标范围内的时间增加了10.87%[95%可信区间9.38%至12.37%;p<0.0001,I²=87%],糖化血红蛋白降低了0.37%(4.77mmol/mol)[95%可信区间-0.49%(-6.39mmol/mol)至-0.26%(-3.14mmol/mol);p<0.0001,I²=77%]。AID系统减少了夜间低血糖、低血糖和高血糖的时间,并改善了患者的困扰,同时DKA或严重低血糖的风险没有增加。在治疗满意度或低血糖恐惧方面未发现差异。在儿童中,使用AID系统或常规治疗在血糖变异性或低血糖持续时间方面没有差异。在敏感性分析中,结果与支持AID的总体分析一致。
无论技术或临床差异如何,使用AID系统超过12周可改善T1DM成人和儿童的血糖结局和糖尿病困扰,且不增加不良事件的风险。