Department of Medicine, Karolinska University Hospital Huddinge, Karolinska Institute, 141 86, Stockholm, Sweden.
Department of Medicine, Clinica Diabetologica, Gijon, Spain.
Diabetologia. 2018 Mar;61(3):539-550. doi: 10.1007/s00125-017-4527-5. Epub 2017 Dec 23.
AIMS/HYPOTHESIS: Evidence for the effectiveness of interstitial glucose monitoring in individuals with type 1 diabetes using multiple daily injection (MDI) therapy is limited. In this pre-specified subgroup analysis of the Novel Glucose-Sensing Technology and Hypoglycemia in Type 1 Diabetes: a Multicentre, Non-masked, Randomised Controlled Trial' (IMPACT), we assessed the impact of flash glucose technology on hypoglycaemia compared with capillary glucose monitoring.
This multicentre, prospective, non-masked, RCT enrolled adults from 23 European diabetes centres. Individuals were eligible to participate if they had well-controlled type 1 diabetes (diagnosed for ≥5 years), HbA ≤ 58 mmol/mol [7.5%], were using MDI therapy and on their current insulin regimen for ≥3 months, reported self-monitoring of blood glucose on a regular basis (equivalent to ≥3 times/day) for ≥2 months and were deemed technically capable of using flash glucose technology. Individuals were excluded if they were diagnosed with hypoglycaemia unawareness, had diabetic ketoacidosis or myocardial infarction in the preceding 6 months, had a known allergy to medical-grade adhesives, used continuous glucose monitoring (CGM) within the previous 4 months or were currently using CGM or sensor-augmented pump therapy, were pregnant or planning pregnancy or were receiving steroid therapy for any disorders. Following 2 weeks of blinded (to participants and investigator) sensor wear by all participants, participants with sensor data for more than 50% of the blinded wear period (or ≥650 individual sensor results) were randomly assigned, in a 1:1 ratio by a central interactive web response system (IWRS) using the biased-coin minimisation method, to flash sensor-based glucose monitoring (intervention group) or self-monitoring of capillary blood glucose (control group). The control group had two further 14 day blinded sensor-wear periods at the 3 and 6 month time points. Participants, investigators and staff were not masked to group allocation. The primary outcome was the change in time in hypoglycaemia (<3.9 mmol/l) between baseline and 6 months in the full analysis set.
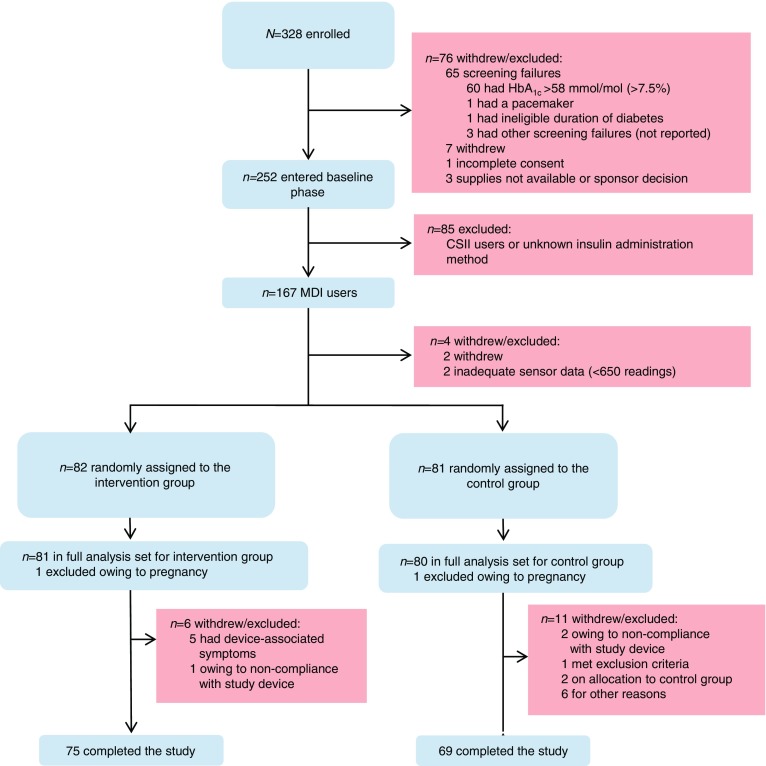
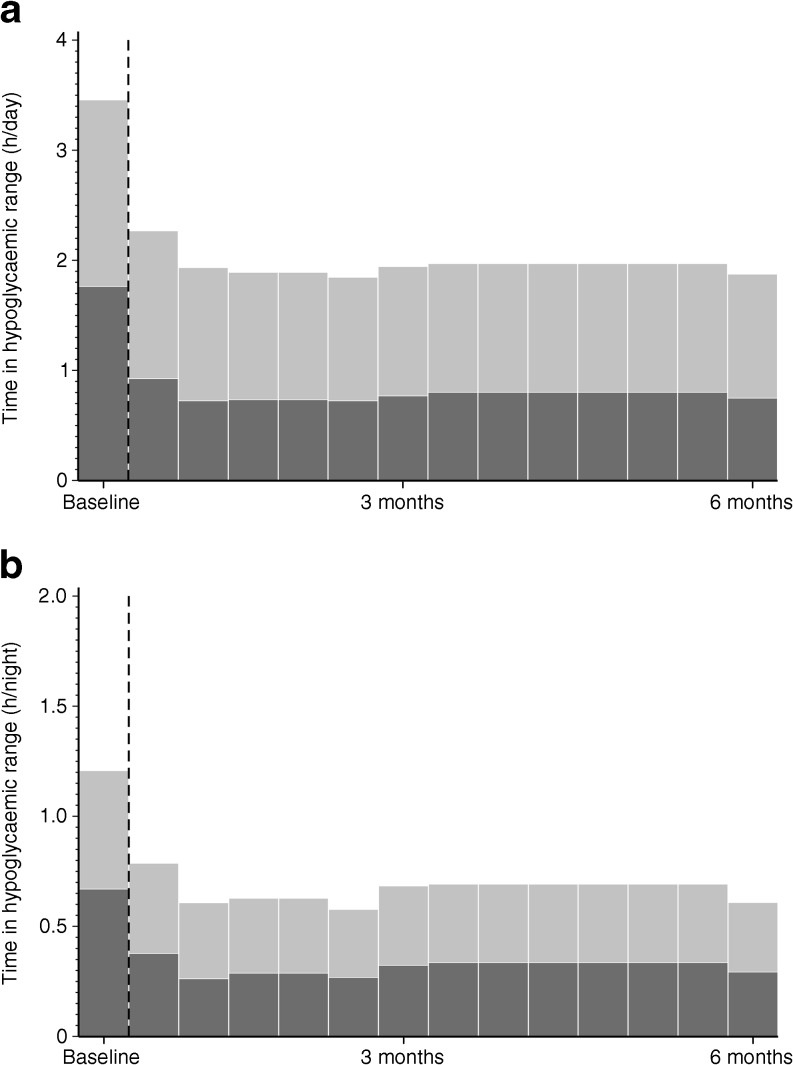
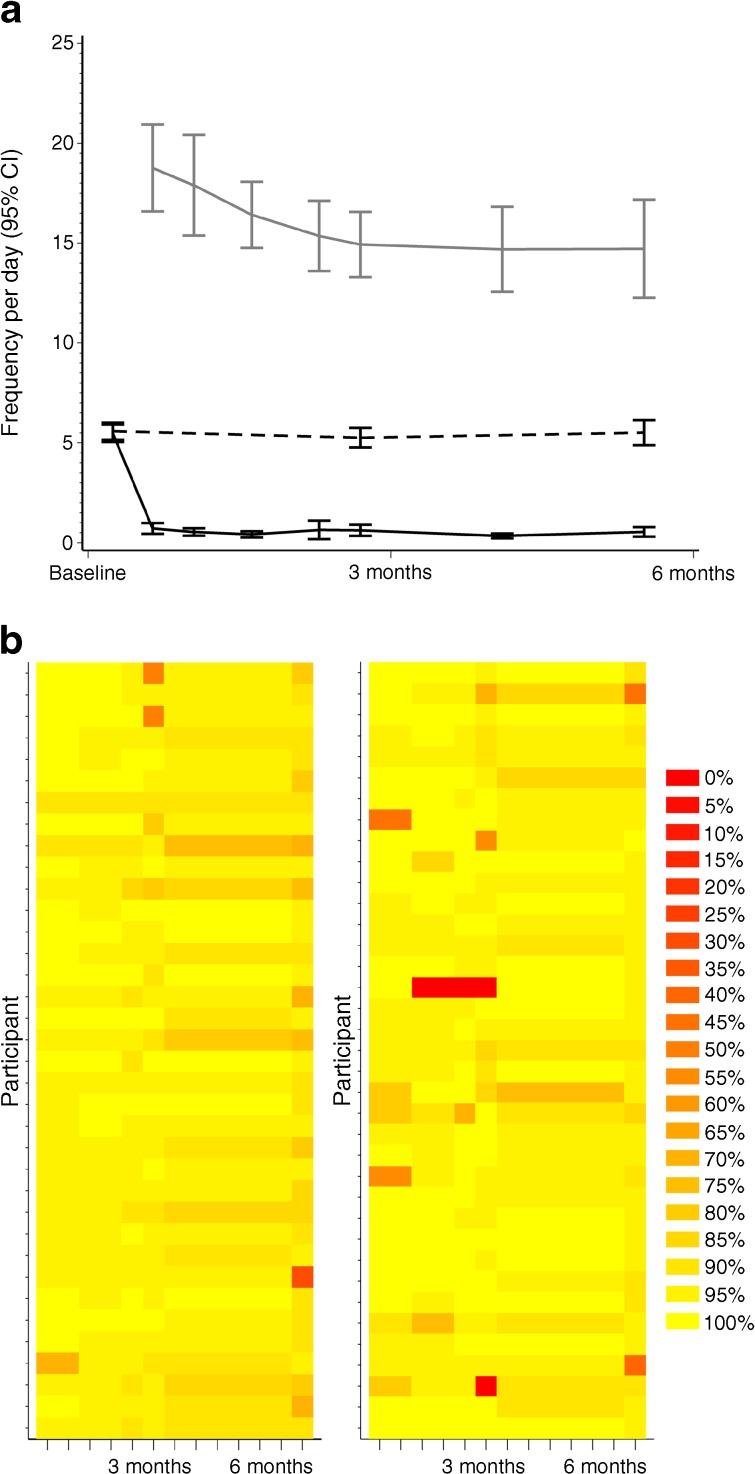
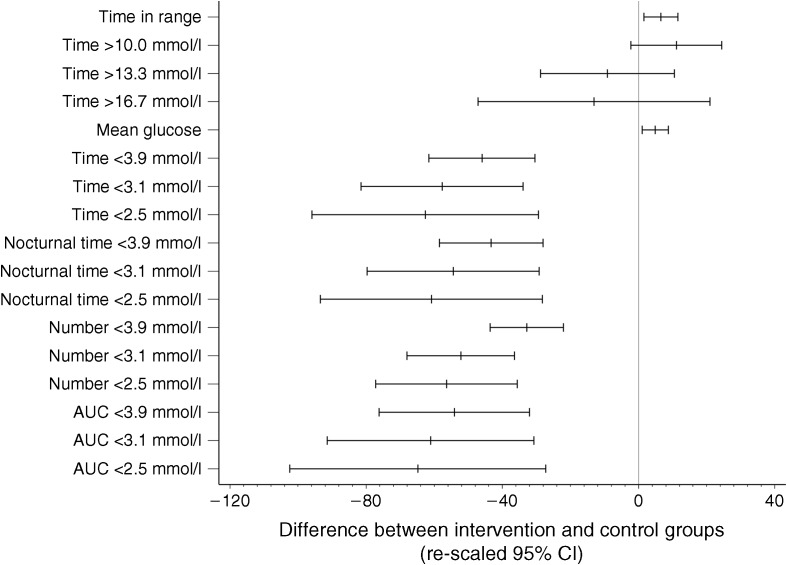
Between 4 September 2014 and 12 February 2015, 167 participants using MDI were enrolled. After screening and the baseline phase, participants were randomised to intervention (n = 82) and control groups (n = 81). One woman from each group was excluded owing to pregnancy; the full analysis set included 161 randomised participants. At 6 months, mean time in hypoglycaemia was reduced by 46.0%, from 3.44 h/day to 1.86 h/day in the intervention group (baseline adjusted mean change, -1.65 h/day), and from 3.73 h/day to 3.66 h/day in the control group (baseline adjusted mean change, 0.00 h/day), with a between-group difference of -1.65 (95% CI -2.21, -1.09; p < 0.0001). For participants in the intervention group, the mean ± SD daily sensor scanning frequency was 14.7 ± 10.7 (median 12.3) and the mean number of self-monitored blood glucose tests performed per day reduced from 5.5 ± 2.0 (median 5.4) at baseline to 0.5 ± 1.0 (median 0.1). The baseline frequency of self-monitored blood glucose tests by control participants was maintained (from 5.6 ± 1.9 [median 5.2] to 5.5 ± 2.6 [median 5.1] per day). Treatment satisfaction and perception of hypo/hyperglycaemia were improved compared with control. No device-related hypoglycaemia or safety-related issues were reported. Nine serious adverse events were reported for eight participants (four in each group), none related to the device. Eight adverse events for six of the participants in the intervention group were also reported, which were related to sensor insertion/wear; four of these participants withdrew because of the adverse event.
CONCLUSIONS/INTERPRETATION: Use of flash glucose technology in type 1 diabetes controlled with MDI therapy significantly reduced time in hypoglycaemia without deterioration of HbA, and improved treatment satisfaction.
ClinicalTrials.gov NCT02232698 FUNDING: Abbott Diabetes Care, Witney, UK.
目的/假设:使用多次每日注射(MDI)疗法的 1 型糖尿病患者中,间歇性葡萄糖监测的有效性证据有限。在“1 型糖尿病中新型葡萄糖感应技术和低血糖:一项多中心、非盲、随机对照试验(IMPACT)”的预先指定亚组分析中,我们评估了与毛细血管血糖监测相比,闪存血糖技术对低血糖的影响。
这项多中心、前瞻性、非盲、随机对照 RCT 招募了来自 23 个欧洲糖尿病中心的成年人。如果患者符合以下条件,则有资格参与研究:1 型糖尿病确诊时间超过 5 年;HbA1c≤58mmol/mol[7.5%];使用 MDI 治疗;当前胰岛素方案已使用≥3 个月;自我监测血糖定期进行(相当于≥3 次/天)≥2 个月;并且被认为有能力使用闪存血糖技术。如果患者患有低血糖无意识、在过去 6 个月内患有糖尿病酮症酸中毒或心肌梗死、对医用级粘合剂过敏、在过去 4 个月内使用连续血糖监测(CGM)或目前正在使用 CGM 或传感器增强型泵治疗、怀孕或计划怀孕或正在接受任何疾病的类固醇治疗,则将被排除在外。在所有参与者佩戴传感器进行为期 2 周的盲法(对参与者和研究者)后,对于在盲法佩戴期内有超过 50%的传感器数据(或≥650 个单独传感器结果)的参与者,使用中央交互网络响应系统(IWRS),按照偏置硬币最小化方法,以 1:1 的比例随机分配到基于闪存传感器的血糖监测(干预组)或毛细血管血糖自我监测(对照组)。对照组在 3 个月和 6 个月时还有另外两个 14 天的盲法传感器佩戴期。参与者、研究者和工作人员对分组分配不知情。主要结局是在基线和 6 个月时,低血糖(<3.9mmol/l)时间在全分析集中的变化。
在 2014 年 9 月 4 日至 2015 年 2 月 12 日期间,共有 167 名使用 MDI 的参与者被纳入研究。经过筛选和基线期后,参与者被随机分配到干预组(n=82)和对照组(n=81)。每组各有一名女性因怀孕而被排除;全分析集包括 161 名随机参与者。在 6 个月时,干预组的低血糖时间平均减少了 46.0%,从基线时的 3.44 小时/天减少到 1.86 小时/天(基线调整后的平均变化,-1.65 小时/天),对照组的低血糖时间从 3.73 小时/天减少到 3.66 小时/天(基线调整后的平均变化,0.00 小时/天),两组之间的差异为-1.65(95%CI-2.21,-1.09;p<0.0001)。对于干预组的参与者,平均±SD 每日传感器扫描频率为 14.7±10.7(中位数 12.3),每日自我监测血糖测试次数从基线时的 5.5±2.0(中位数 5.4)减少到 0.5±1.0(中位数 0.1)。对照组参与者的自我监测血糖测试频率保持不变(从 5.6±1.9[中位数 5.2]到 5.5±2.6[中位数 5.1])。与对照组相比,治疗满意度和对高/低血糖的感知得到了改善。没有报告与设备相关的低血糖或安全相关问题。有 8 名参与者报告了 9 例严重不良事件(每组 4 例),均与设备无关。干预组的 6 名参与者还报告了 8 例不良事件,这些事件与传感器插入/佩戴有关;其中 4 名参与者因不良事件而退出。
结论/解释:在 MDI 治疗控制的 1 型糖尿病患者中使用闪存血糖技术显著减少了低血糖时间,而 HbA1c 没有恶化,并且提高了治疗满意度。
ClinicalTrials.gov NCT02232698 基金:Abbott Diabetes Care,英国威茨尼。