Department of Obstetrics and Gynecology, Hospital Universitario de Torrejón, Torrejón de Ardoz, 28850 Madrid, Spain.
Faculty of Medicine, Universidad Francisco de Vitoria, Pozuelo de Alarcón, 28223 Madrid, Spain.
Medicina (Kaunas). 2023 Sep 15;59(9):1670. doi: 10.3390/medicina59091670.
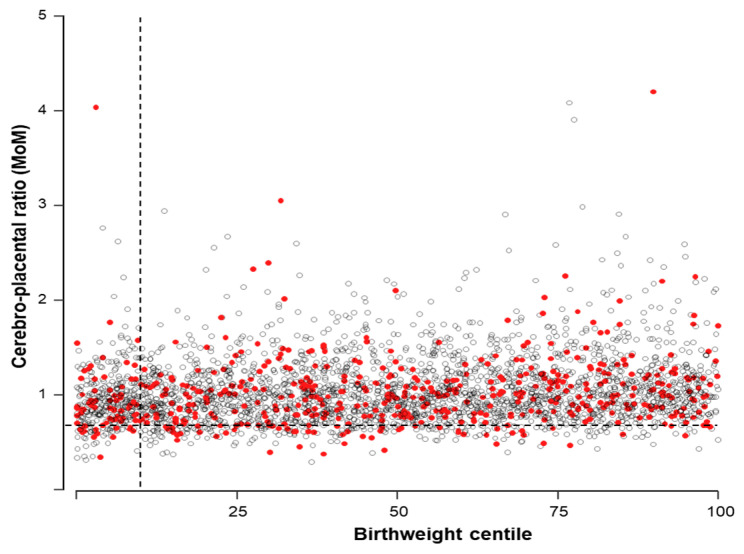
Over the last few years, great interest has arisen in the role of the cerebroplacental ratio (CPR) to identify low-risk pregnancies at higher risk of adverse pregnancy outcomes. This study aimed to assess the predictive capacity of the CPR for adverse perinatal outcomes in all uncomplicated singleton pregnancies attending an appointment at 40-42 weeks. : This is a retrospective cohort study including all consecutive singleton pregnancies undergoing a routine prenatal care appointment after 40 weeks in three maternity units in Spain and the United Kingdom from January 2017 to December 2019. The primary outcome was adverse perinatal outcomes defined as stillbirth or neonatal death, cesarean section or instrumental delivery due to fetal distress during labor, umbilical arterial cord blood pH < 7.0, umbilical venous cord blood pH < 7.1, Apgar score at 5 min < 7, and admission to the neonatal unit. Logistic mixed models and ROC curve analyses were used to analyze the data. A total of 3143 pregnancies were analyzed, including 537 (17.1%) with an adverse perinatal outcome. Maternal age (odds ratio (OR) 1.03, 95% confidence interval (CI) 1.01 to 1.04), body mass index (OR 1.04, 95% CI 1.03 to 1.06), racial origin (OR 2.80, 95% CI 1.90 to 4.12), parity (OR 0.36, 95% CI 0.29 to 0.45), and labor induction (OR 1.79, 95% CI 1.36 to 2.35) were significant predictors of adverse perinatal outcomes with an area under the ROC curve of 0.743 (95% CI 0.720 to 0.766). The addition of the CPR to the previous model did not improve performance. Additionally, the CPR alone achieved a detection rate of only 11.9% (95% CI 9.3 to 15) when using the 10th centile as the screen-positive cutoff. Our data on late-term unselected pregnancies suggest that the CPR is a poor predictor of adverse perinatal outcomes.
在过去的几年中,人们对胎脑比(CPR)在识别具有不良妊娠结局风险的低危妊娠中的作用产生了浓厚的兴趣。本研究旨在评估 CPR 在所有 40-42 周就诊的无并发症单胎妊娠中的不良围产结局的预测能力。
这是一项回顾性队列研究,纳入了 2017 年 1 月至 2019 年 12 月期间,西班牙和英国三个产科单位中所有接受常规产前检查的连续单胎妊娠。主要结局是不良围产结局,定义为死胎或新生儿死亡、因产程中胎儿窘迫而行剖宫产术或器械助产、脐动脉脐带血 pH 值<7.0、脐静脉脐带血 pH 值<7.1、5 分钟 Apgar 评分<7 分和新生儿病房收治。使用逻辑混合模型和 ROC 曲线分析数据。共分析了 3143 例妊娠,其中 537 例(17.1%)发生不良围产结局。产妇年龄(比值比(OR)1.03,95%置信区间(CI)1.01 至 1.04)、体重指数(OR 1.04,95%CI 1.03 至 1.06)、种族(OR 2.80,95%CI 1.90 至 4.12)、产次(OR 0.36,95%CI 0.29 至 0.45)和引产(OR 1.79,95%CI 1.36 至 2.35)是不良围产结局的显著预测因素,ROC 曲线下面积为 0.743(95%CI 0.720 至 0.766)。将 CPR 添加到之前的模型中并不能提高性能。此外,当使用第 10 百分位数作为筛查阳性截断值时,CPR 单独使用的检出率仅为 11.9%(95%CI 9.3 至 15)。
我们关于晚期未选择妊娠的数据表明,CPR 是不良围产结局的预测能力较差。