Department of Obstetrics and Gynaecology, Reproduction and Development, Amsterdam UMC, Vrije Universiteit Amsterdam, Amsterdam, The Netherlands.
Department of Epidemiology and Biostatistics, Amsterdam UMC, Vrije Universiteit Amsterdam, Amsterdam, The Netherlands.
BJOG. 2021 Jan;128(2):226-235. doi: 10.1111/1471-0528.16287. Epub 2020 Jun 8.
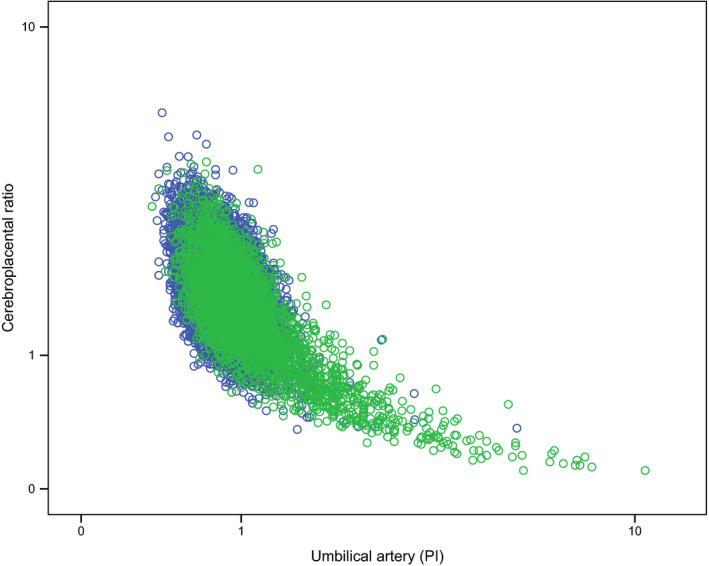
To investigate if cerebroplacental ratio (CPR) adds to the predictive value of umbilical artery pulsatility index (UA PI) alone - standard of practice - for adverse perinatal outcome in singleton pregnancies.
Meta-analysis based on individual participant data (IPD).
Ten centres provided 17 data sets for 21 661 participants, 18 731 of which could be included. Sample sizes per data set ranged from 207 to 9215 individuals. Patient populations varied from uncomplicated to complicated pregnancies.
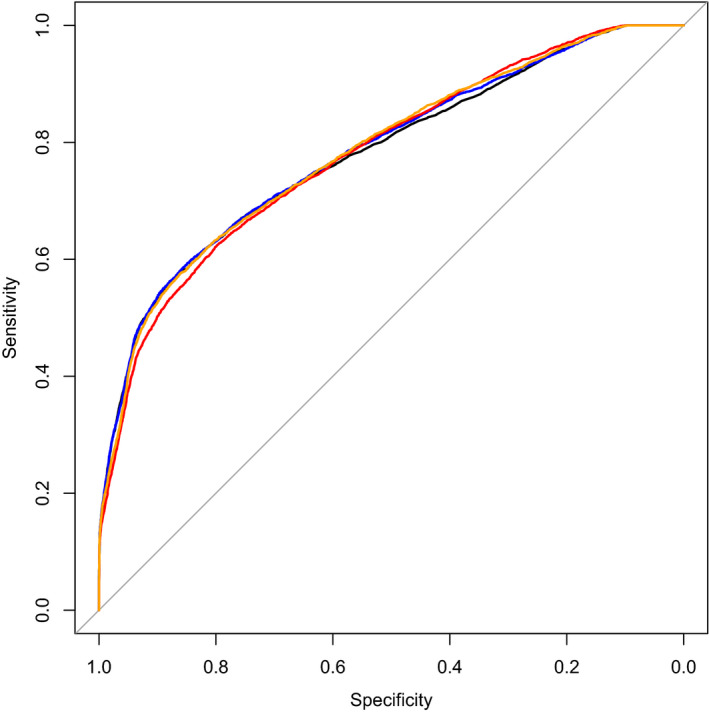
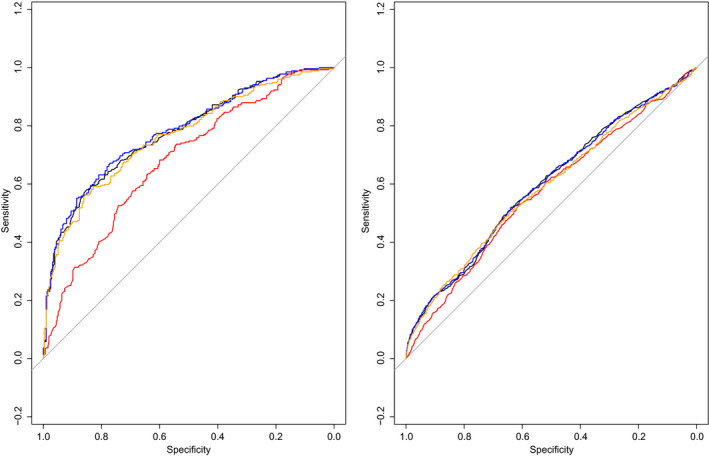
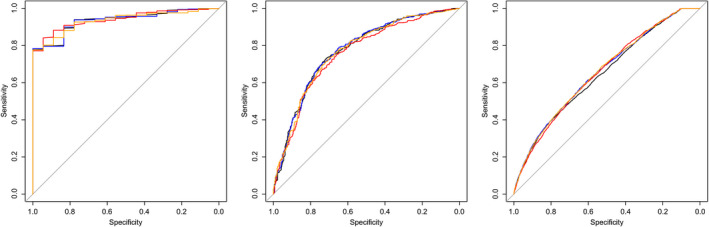
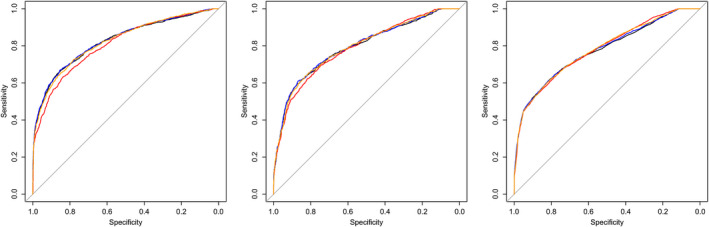
In a collaborative, pooled analysis, we compared the prognostic value of combining CPR with UA PI, versus UA PI only and CPR only, with a one-stage IPD approach. After multiple imputation of missing values, we used multilevel multivariable logistic regression to develop prediction models. We evaluated the classification performance of all models with receiver operating characteristics analysis. We performed subgroup analyses according to gestational age, birthweight centile and estimated fetal weight centile.
Composite adverse perinatal outcome, defined as perinatal death, caesarean section for fetal distress or neonatal unit admission.
Adverse outcomes occurred in 3423 (18%) participants. The model with UA PI alone resulted in an area under the curve (AUC) of 0.775 (95% CI 0.709-0.828) and with CPR alone in an AUC of 0.778 (95% CI 0.715-0.831). Addition of CPR to the UA PI model resulted in an increase in the AUC of 0.003 points (0.778, 95% CI 0.714-0.831). These results were consistent across all subgroups.
Cerebroplacental ratio added no predictive value for adverse perinatal outcome beyond UA PI, when assessing singleton pregnancies, irrespective of gestational age or fetal size.
Doppler measurement of cerebroplacental ratio in clinical practice has limited added predictive value to umbilical artery alone.
研究脑-胎盘比值 (CPR) 是否能增加脐动脉搏动指数 (UA PI) 的预测价值,因为后者是目前的标准实践,用于预测单胎妊娠的不良围产结局。
基于个体参与者数据的荟萃分析 (IPD)。
10 个中心提供了 17 个数据集,共有 21661 名参与者,其中 18731 名可以纳入分析。每个数据集的样本量范围从 207 到 9215 人不等。患者人群从简单的妊娠到复杂的妊娠不等。
在协作的、汇集的分析中,我们使用 IPD 方法比较了将 CPR 与 UA PI 相结合、仅使用 UA PI 或仅使用 CPR 的预测价值。在对缺失值进行多次插补后,我们使用多级多变量逻辑回归来建立预测模型。我们使用接收者操作特征分析来评估所有模型的分类性能。我们根据胎龄、出生体重百分位数和估计胎儿体重百分位数进行亚组分析。
复合不良围产结局,定义为围产儿死亡、因胎儿窘迫行剖宫产术或新生儿重症监护病房入院。
3423 名(18%)参与者发生不良结局。单独使用 UA PI 的模型的曲线下面积 (AUC) 为 0.775(95% CI 0.709-0.828),单独使用 CPR 的 AUC 为 0.778(95% CI 0.715-0.831)。将 CPR 添加到 UA PI 模型中,AUC 增加了 0.003 个点(0.778,95% CI 0.714-0.831)。这些结果在所有亚组中都是一致的。
在评估单胎妊娠时,CPR 对 UA PI 评估不良围产结局的预测价值没有增加,无论胎龄或胎儿大小如何。
在临床实践中,多普勒测量脑-胎盘比值对单独使用脐动脉的预测价值有限。