Kaemmerer Ann-Sophie, Ciotola Francesco, Geißdörfer Walter, Harig Frank, Mattner Jochen, Seitz Timo, Suleiman Mathieu N, Weyand Michael, Heim Christian
Department of Cardiac Surgery, University Hospital Erlangen, Friedrich-Alexander-University Erlangen-Nürnberg, D-91054 Erlangen, Germany.
Department of Cardiology and Pneumonology (Med 1), Klinikum Fürth, Academic Teaching Hospital of the Friedrich-Alexander-University Erlangen-Nürnberg, D-90766 Fürth, Germany.
Pathogens. 2023 Sep 4;12(9):1130. doi: 10.3390/pathogens12091130.
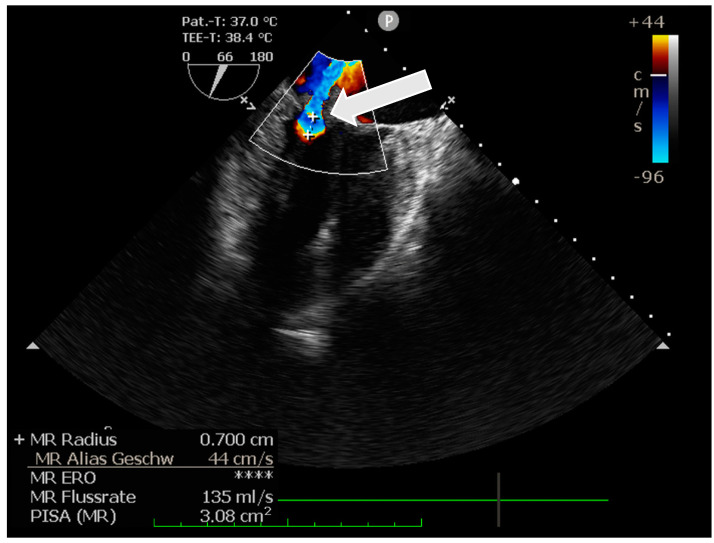
Infective endocarditis (IE) is still a life-threatening disease with high morbidity and mortality. While usually caused by a single bacterium, poly-microbial infective endocarditis (IE) is rare. Here, we report a (blood-culture-negative) dual pathogen mitral valve IE caused by and : A 53-year-old woman was presented to an internal medicine department with abdominal pain for further evaluation. Within the diagnostic work up, transthoracic echocardiography (TTE) revealed an irregularly shaped echogenic mass (5 × 13 mm) adherent to the edge of the posterior mitral valve leaflet and protruding into the left atrium. As infected endocarditis was suspected, blood cultures were initially obtained, but they remained negative. Chronic Q fever infection was diagnosed using serologic testing. After the occurrence of cerebral thromboembolic events, the patient was admitted for mitral valve surgery. Intraoperatively, a massively destructed mitral valve with adhering vegetations was noted. Examination of the mitral valve by broad-range bacterial polymerase chain reaction (PCR) and amplicon sequencing confirmed infection and yielded as the second pathogen. Based on the detailed diagnosis, appropriate antibiotic therapy of both pathogens was initiated, and the patient could be discharged uneventfully on the 11th postoperative day after a successful minimal-invasive mitral valve replacement.
感染性心内膜炎(IE)仍然是一种具有高发病率和死亡率的危及生命的疾病。虽然通常由单一细菌引起,但多微生物感染性心内膜炎(IE)很少见。在此,我们报告一例由 和 引起的(血培养阴性)双病原体二尖瓣IE:一名53岁女性因腹痛就诊于内科进行进一步评估。在诊断检查过程中,经胸超声心动图(TTE)显示一个不规则形状的回声团块(5×13mm)附着于二尖瓣后叶边缘并突入左心房。由于怀疑为感染性心内膜炎,最初进行了血培养,但结果为阴性。通过血清学检测诊断为慢性Q热感染。在发生脑栓塞事件后,患者入院接受二尖瓣手术。术中发现二尖瓣严重破坏并伴有赘生物附着。通过广谱细菌聚合酶链反应(PCR)和扩增子测序对二尖瓣进行检查,证实了 感染,并鉴定出 为第二种病原体。基于详细诊断,开始对两种病原体进行适当的抗生素治疗,患者在成功进行微创二尖瓣置换术后第11天顺利出院。