Department of Obstetrics and Gynaecology, Institute of Clinical Science, Sahlgrenska Academy, Gothenburg University, Gothenburg, Sweden.
Reproductive Medicine, Sahlgrenska University Hospital, Gothenburg, Sweden.
Front Endocrinol (Lausanne). 2023 Sep 11;14:1239702. doi: 10.3389/fendo.2023.1239702. eCollection 2023.
To investigate the association between female body mass index (BMI) and live birth rates and maternal and perinatal outcomes after fertilization (IVF).
We performed a national, population-based cohort study including women undergoing IVF between 2002 and 2020. The cohort included 126,620 fresh cycles and subsequent frozen embryo transfers between 2007 and 2019 (subpopulation 1) and 58,187 singleton deliveries between 2002 and 2020 (subpopulation 2). Exposure was female BMI (kg/m) categorized according to the World Health Organization as underweight (<18.5), normal weight (18.5-24.9, reference), overweight (25.0-29.9), class I obesity (30.0-34.9), class II obesity (35.0-39.9), and class III obesity (≥40.0). The primary outcome in subpopulation 1 was cumulative live birth per started fresh IVF cycle, including fresh and subsequent frozen embryo transfers. Primary outcomes in subpopulation 2 were hypertensive disorders of pregnancy and preterm birth at less than 37 weeks. Risk ratios (RRs) with 95% confidence intervals (CIs) for the association between BMI class and outcomes were calculated using generalized linear models after adjustment for relevant confounders.
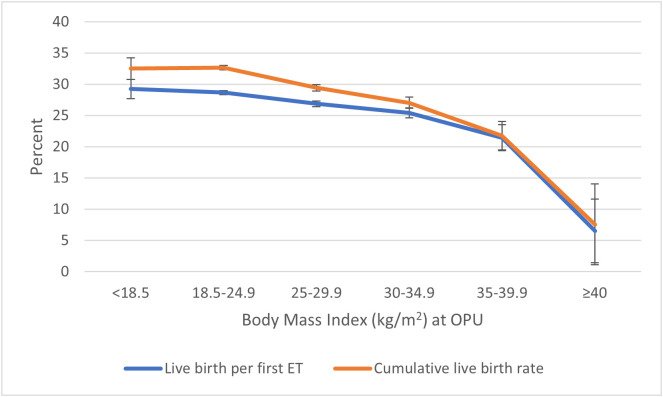
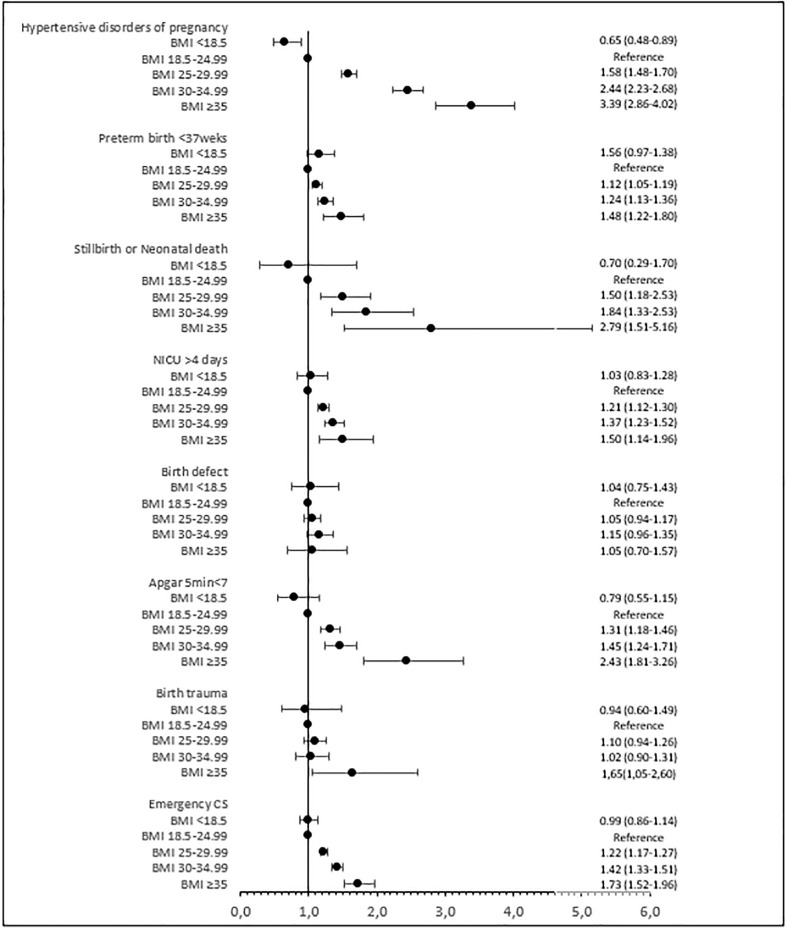
The cumulative live birth rate decreased significantly with increasing BMI from 32.6% in normal-weight women to 29.4% in overweight women, 27.0% in women in obesity class I, 21.8% in women in obesity class II, and 7.6% in women in obesity class III. The risk of hypertensive disorders of pregnancy increased significantly and progressively with increasing BMI, from 4.6% in normal-weight women to 7.8% in overweight women and 12.5%, 17.9%, and 20.3% in women in obesity classes I, II, and III. The risk of preterm birth followed a similar pattern, from 6.3% in normal-weight women to 7.5% in overweight women and 8.9%, 9.9%, and 15.3% in women in obesity classes I, II, and III. The risks of other perinatal complications, such as perinatal death, showed an even more pronounced increase.
Using a large and complete national cohort of women undergoing IVF, we demonstrate a dose-dependent decrease in live birth rate and a substantial increase in maternal and perinatal complications with increasing BMI. Strategies to improve this situation are warranted.
探讨女性体重指数(BMI)与体外受精(IVF)后活产率和母婴围生结局的关系。
我们进行了一项全国性、基于人群的队列研究,纳入了 2002 年至 2020 年期间接受 IVF 的女性。该队列包括 2007 年至 2019 年期间的 126620 个新鲜周期和随后的冷冻胚胎移植(亚群 1)以及 2002 年至 2020 年期间的 58187 例单胎分娩(亚群 2)。根据世界卫生组织的标准,将女性 BMI(kg/m)分为消瘦(<18.5)、正常体重(18.5-24.9,参考值)、超重(25.0-29.9)、I 度肥胖(30.0-34.9)、II 度肥胖(35.0-39.9)和 III 度肥胖(≥40.0)。亚群 1 的主要结局是每个起始新鲜 IVF 周期的累积活产率,包括新鲜周期和随后的冷冻胚胎移植。亚群 2 的主要结局是妊娠高血压疾病和早产(<37 周)。使用广义线性模型,在调整相关混杂因素后,计算 BMI 类别与结局之间的风险比(RR)及其 95%置信区间(CI)。
随着 BMI 的增加,从正常体重女性的 32.6%到超重女性的 29.4%、肥胖 I 度女性的 27.0%、肥胖 II 度女性的 21.8%和肥胖 III 度女性的 7.6%,累积活产率显著下降。随着 BMI 的增加,妊娠高血压疾病的风险显著且逐渐增加,从正常体重女性的 4.6%增加到超重女性的 7.8%以及肥胖 I 度、II 度和 III 度女性的 12.5%、17.9%和 20.3%。早产的风险也呈现出类似的模式,从正常体重女性的 6.3%增加到超重女性的 7.5%以及肥胖 I 度、II 度和 III 度女性的 8.9%、9.9%和 15.3%。其他围生期并发症(如围生儿死亡)的风险甚至更显著增加。
本研究使用大型、完整的全国性 IVF 女性队列,证明了活产率随着 BMI 的增加而呈剂量依赖性下降,母婴围生期并发症显著增加。需要采取策略来改善这种情况。