The Ottawa Hospital Cancer Centre, Ottawa, Ontario, Canada.
International Atomic Energy Agency, Vienna, Austria.
JCO Glob Oncol. 2023 Sep;9:e2300130. doi: 10.1200/GO.23.00130.
Sufficient radiotherapy (RT) capacity is essential to delivery of high-quality cancer care. However, despite sufficient capacity, universal access is not always possible in high-income countries because of factors beyond the commonly used parameter of machines per million people. This study assesses the barriers to RT in a high-income country and how these affect cancer mortality.
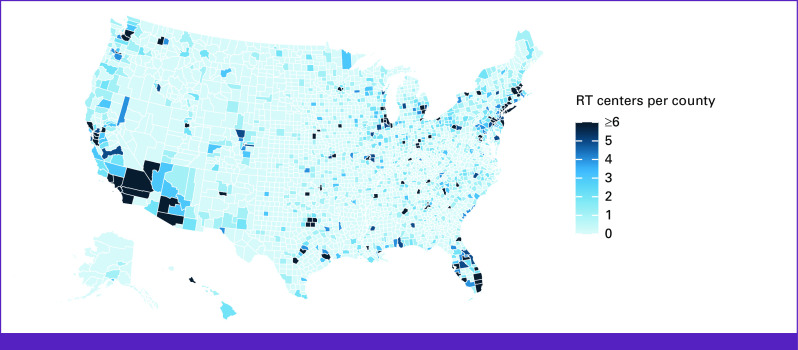
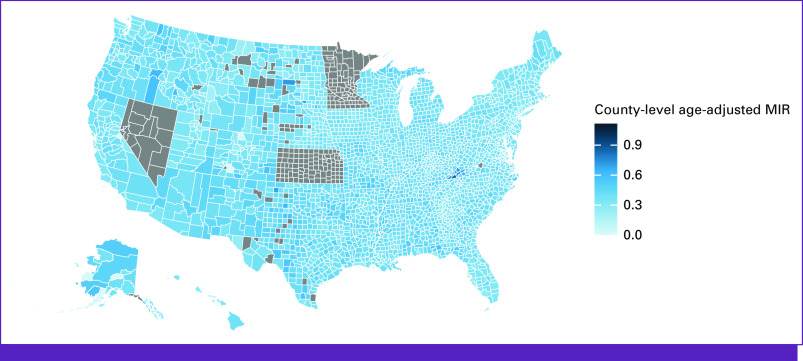
This cross-sectional study used US county-level data obtained from Center for Disease Control and Prevention and the International Atomic Energy Agency Directory of Radiotherapy Centres. RT facilities in the United States were mapped using Geographic Information Systems software. Univariate analysis was used to identify whether distance to a RT center or various socioeconomic factors were predictive of all-cancer mortality-to-incidence ratio (MIR). Significant variables ( ≤ .05) on univariate analysis were included in a step-wise backward elimination method of multiple regression analysis.
Thirty-one percent of US counties have at least one RT facility and 8.3% have five or more. The median linear distance from a county's centroid to the nearest RT center was 36 km, and the median county all-cancer MIR was 0.37. The amount of RT centers, linear accelerators, and brachytherapy units per 1 million people were associated with all-cancer MIR ( < .05). Greater distance to RT facilities, lower county population, lower average income per county, and higher proportion of patients without health insurance were associated with increased all-cancer MIR (-squared, 0.2113; , 94.22; < .001).
This analysis used unique high-quality data sets to identify significant barriers to RT access that correspond to higher cancer mortality at the county level. Geographic access, personal income, and insurance status all contribute to these concerning disparities. Efforts to address these barriers are needed.
充足的放射治疗(RT)能力对于提供高质量的癌症护理至关重要。然而,尽管有足够的能力,但在高收入国家,由于普遍使用的每百万人拥有机器数量之外的因素,并非总能实现普遍获得 RT 的机会。本研究评估了高收入国家 RT 的障碍以及这些障碍如何影响癌症死亡率。
本横断面研究使用了美国县一级的数据,这些数据来自疾病控制和预防中心以及国际原子能机构放射治疗中心目录。使用地理信息系统软件对美国的 RT 设施进行了绘图。单变量分析用于确定距离 RT 中心的距离或各种社会经济因素是否可预测所有癌症死亡率与发病率比(MIR)。单变量分析中具有统计学意义的变量(≤0.05)被纳入逐步向后消除多元回归分析方法。
31%的美国县至少有一个 RT 设施,8.3%的县有 5 个或更多 RT 设施。从县中心点到最近 RT 中心的中位数线性距离为 36 公里,县内所有癌症的中位数 MIR 为 0.37。每百万人拥有的 RT 中心、线性加速器和近距离放射治疗单位的数量与所有癌症的 MIR 相关(<0.05)。与 RT 设施的距离较远、县人口较少、县人均收入较低以及没有医疗保险的患者比例较高与所有癌症 MIR 增加相关(平方和,0.2113;自由度,94.22;<0.001)。
本分析使用了独特的高质量数据集,确定了 RT 获得的重大障碍,这些障碍与县一级更高的癌症死亡率相对应。地理可达性、个人收入和保险状况都促成了这些令人担忧的差异。需要努力解决这些障碍。