Division of Pathology, IEO European Institute of Oncology IRCCS, 20141, Milan, Italy.
Department of Oncology and Hemato-Oncology, University of Milan, 20122, Milan, Italy.
Virchows Arch. 2024 Jan;484(1):3-14. doi: 10.1007/s00428-023-03656-w. Epub 2023 Sep 28.
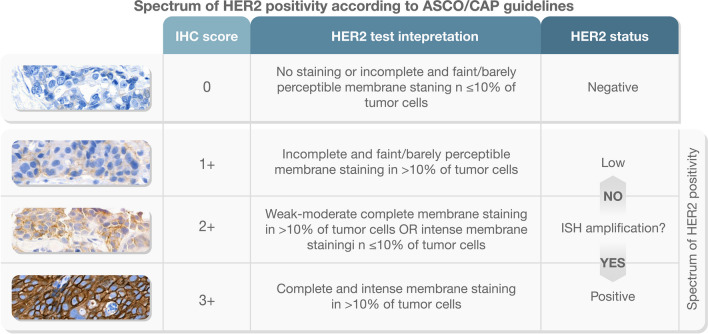
Since the release of the DESTINY-Breast04 (DB-04) trial findings in June 2022, the field of pathology has seen a renaissance of HER2 as a predictive biomarker in breast cancer. The trial focused on patients with metastatic breast cancer who were classified as "HER2-low," i.e., those with immunohistochemistry (IHC) HER2 1 + or 2 + and negative in situ hybridization (ISH) results. The study revealed that treating these patients with trastuzumab deruxtecan (T-DXd) instead of the oncologist's chosen chemotherapy led to outstanding improvements in survival. This has challenged the existing binary HER2 pathological classification system, which categorized tumors as either positive (overexpression/amplification) or negative, as per the ASCO/CAP 2018 guideline reaffirmed by ASCO/CAP 2023 guideline update. Given that DB-04 excluded patients with HER2 IHC score 0 status, the results of the ongoing DB-06 trial may shed further light on the potential benefits of T-DXd therapy for these patients. Roughly half of all breast cancers are estimated to belong to the HER2-low category, which does not represent a distinct or specific subtype of cancer. Instead, it encompasses a diverse group of tumors that exhibit clinical, morphological, immunohistochemical, and molecular variations. However, HER2-low offers a distinctive biomarker status that identifies a specific therapeutic regimen (i.e., T-DXd) linked to a favorable prognosis in breast cancer. This unique association emphasizes the importance of accurately identifying these tumors. Differentiating between a HER2 IHC score 0 and score 1 + has not been clinically significant until now. To ensure accurate classification and avoid misdiagnosis, it is necessary to adopt standardized procedures, guidelines, and specialized training for pathologists in interpreting HER2 expression in the lower spectrum. Additionally, the utilization of artificial intelligence holds promise in supporting this endeavor. Here, we address the current state of the art and unresolved issues in assessing HER2-low status, with a particular emphasis on the score 0. We explore the dilemma surrounding the exclusion of HER2-zero patients from potentially beneficial therapy based on traditional HER2 testing. Additionally, we examine the clinical context, considering that DB-04 primarily involved heavily pretreated late-stage metastatic breast cancers. We also delve into emerging evidence suggesting that extrapolating HER2-low status from the original diagnosis may lead to misleading results. Finally, we provide recommendations for conducting high-quality testing and propose a standardized pathology report in compliance with 2023 ASCO/CAP updates and 2023 ESMO consensus statements on HER2-low breast cancer.
自 2022 年 6 月 DESTINY-Breast04(DB-04)试验结果发布以来,病理学领域对 HER2 作为乳腺癌预测生物标志物的认识发生了重大变化。该试验主要针对转移性乳腺癌患者,这些患者被归类为“HER2-低”,即免疫组化(IHC)HER2 1+或 2+且原位杂交(ISH)结果为阴性。该研究表明,用曲妥珠单抗 deruxtecan(T-DXd)治疗这些患者而不是肿瘤学家选择的化疗可显著提高生存率。这对现有的二元 HER2 病理分类系统提出了挑战,该系统根据 ASCO/CAP 2018 指南和 ASCO/CAP 2023 指南更新重新确认的标准,将肿瘤归类为阳性(过表达/扩增)或阴性。鉴于 DB-04 排除了 HER2 IHC 评分 0 状态的患者,正在进行的 DB-06 试验的结果可能进一步阐明 T-DXd 治疗对这些患者的潜在益处。大约一半的乳腺癌估计属于 HER2-低类别,它不是一种独特或特定的癌症亚型。相反,它包含一组具有临床、形态学、免疫组织化学和分子变异的不同肿瘤。然而,HER2-低提供了一个独特的生物标志物状态,可确定特定的治疗方案(即 T-DXd)与乳腺癌的有利预后相关。这种独特的关联强调了准确识别这些肿瘤的重要性。直到现在,HER2 IHC 评分 0 与评分 1+之间的区别在临床上并不重要。为了确保准确分类和避免误诊,有必要为病理学家采用标准化程序、指南和专门培训来解释较低范围内的 HER2 表达。此外,人工智能的应用有望为这一努力提供支持。在这里,我们讨论了评估 HER2-低状态的当前最新技术和未解决的问题,特别关注评分 0。我们探讨了根据传统 HER2 检测将 HER2-0 患者排除在潜在有益治疗之外的困境。此外,我们还考虑了临床背景,因为 DB-04 主要涉及预处理后的晚期转移性乳腺癌。我们还深入探讨了新出现的证据,表明从最初诊断推断 HER2-低状态可能会导致误导性结果。最后,我们提出了高质量检测的建议,并根据 2023 年 ASCO/CAP 更新和 2023 年 ESMO 关于 HER2-低乳腺癌的共识声明,提出了标准化的病理报告。