Joosten Pien Gabriele Francien, Borgdorff Marieke Paulina, Botman Matthijs, Bouman Mark-Bram, van Embden Daphne, Giannakópoulos Georgios Fredericus
Trauma Unit, Department of Surgery, Amsterdam University Medical Center, Meibergdreef 9, 1105AZ, Amsterdam, The Netherlands.
Department of Plastic, Reconstructive, and Hand Surgery, Amsterdam University Medical Center, Meibergdreef 9, J1A-207, 1105AZ, Amsterdam, The Netherlands.
Eur J Trauma Emerg Surg. 2024 Apr;50(2):467-476. doi: 10.1007/s00068-023-02366-x. Epub 2023 Sep 30.
Guidelines on the management of open tibia fractures recommend timely treatment in a limb reconstruction center which offer joint orthopedic-trauma and plastic surgery services. However, patient's transfer between centers remains inevitable. This review aims to evaluate the clinical outcomes and hospital factors for patients directly admitted and transferred patients to a limb-reconstruction center.
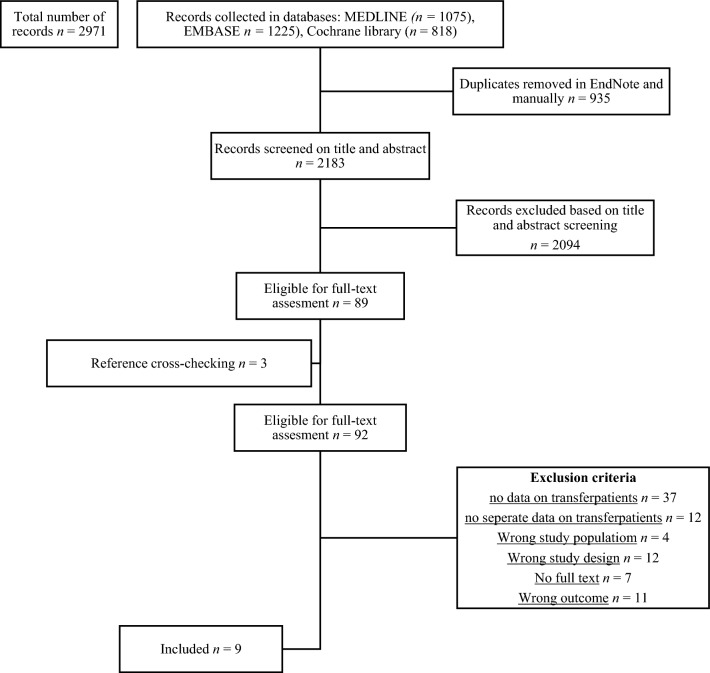
A research protocol adhering to PRISMA standards was established. The search included databases like MEDLINE, EMBASE, and the Cochrane library up until March 2023. Nine articles met the inclusion criteria, focusing on open tibia fractures. Exclusion criteria were experimental studies, animal studies, and case reports. Outcomes of interest were operation and infection rates, nonunion, limb salvage, and the Enneking limb score.
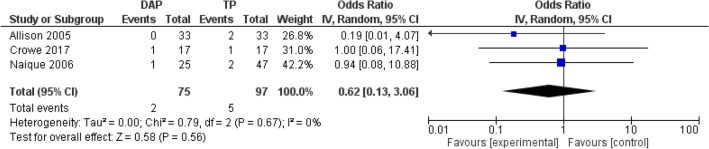
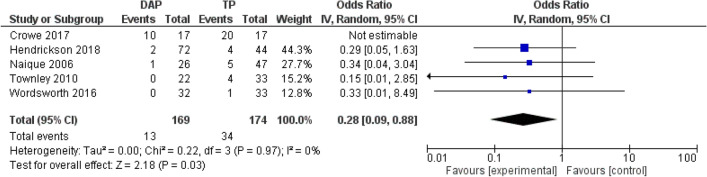
The analysis involved data from 520 patients across nine studies published between 1990 and 2023, with the majority (83.8%) having Gustilo Anderson type III open tibia fractures. Directly admitted patients showed lower overall infection rates (RR 0.30; 95% CI 0.10-0.90; P = 0.03) and fewer deep infections (RR 0.39; 95% CI 0.22-0.68; P = 0.001) compared to transferred patients. Transferred patients experienced an average five-day delay in soft tissue closure and extended hospital stays by eight days. Patients transferred without initial surgical management underwent fewer total surgical procedures. The direct admission group displayed more favorable functional outcomes.
Low- to moderate-quality evidence indicates worse clinical outcomes for transferred patients compared to directly admitted patients. Early treatment in specialized limb reconstruction units is essential for improved results in the management of open tibia fractures.
Therapeutic level IIa.
开放性胫骨骨折治疗指南建议在提供关节骨科创伤和整形手术服务的肢体重建中心进行及时治疗。然而,患者在不同中心之间的转运仍不可避免。本综述旨在评估直接入院患者和转至肢体重建中心的患者的临床结局及医院因素。
制定了一项遵循PRISMA标准的研究方案。检索截至2023年3月的MEDLINE、EMBASE和Cochrane图书馆等数据库。9篇文章符合纳入标准,均聚焦于开放性胫骨骨折。排除标准为实验研究、动物研究和病例报告。感兴趣的结局指标为手术率、感染率、骨不连、肢体挽救情况及Enneking肢体评分。
分析涉及1990年至2023年发表的9项研究中的520例患者数据,其中大多数(83.8%)为Gustilo Anderson III型开放性胫骨骨折。与转院患者相比,直接入院患者的总体感染率较低(RR 0.30;95% CI 0.10 - 0.90;P = 0.03),深部感染较少(RR 0.39;95% CI 0.22 - 0.68;P = 0.001)。转院患者软组织闭合平均延迟5天,住院时间延长8天。未接受初始手术治疗而转院的患者接受的总手术操作较少。直接入院组的功能结局更优。
低至中等质量的证据表明,与直接入院患者相比,转院患者的临床结局更差。在专门的肢体重建单元进行早期治疗对于改善开放性胫骨骨折的治疗效果至关重要。
治疗性IIa级。