Department of Pediatric Nephrology, Perth Children's Hospital, Nedlands, 6009, Australia.
Division of Pediatrics, Medical School, University of Western Australia, Crawley, 6009, Australia.
Pediatr Radiol. 2023 Dec;53(13):2651-2661. doi: 10.1007/s00247-023-05771-x. Epub 2023 Sep 30.
A first febrile urinary tract infection (UTI) is a common condition in children, and pathways of management have evolved over time.
To determine the extent to which pediatricians and surgeons differ in their investigation and management of a first febrile UTI, and to evaluate the justifications for any divergence of approach.
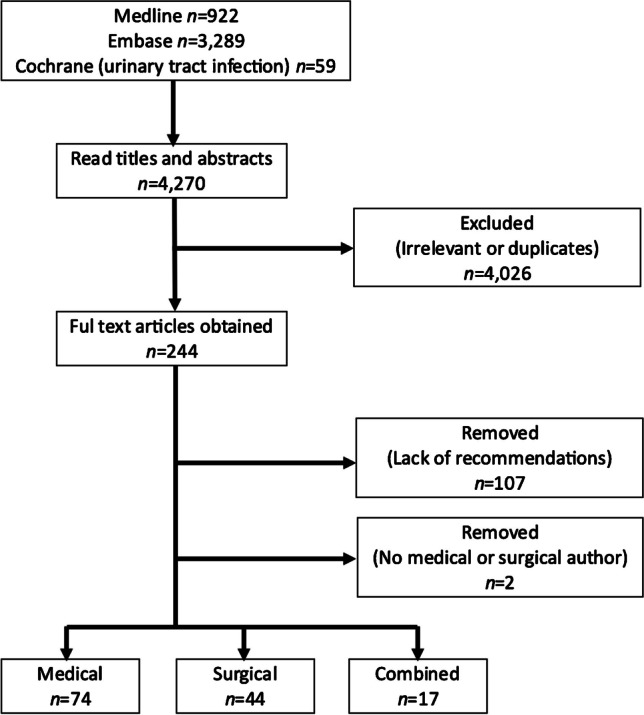
A literature search was conducted for papers addressing investigation and/or management following a first febrile UTI in children published between 2011 and 2021. Searches were conducted on Medline, Embase, and the Cochrane Controlled Trials Register. To be eligible for inclusion, a paper was required to provide recommendations on one or more of the following: ultrasound (US) and voiding cystourethrogram (VCUG), the need for continuous antibiotic prophylaxis and surgery when vesicoureteral reflux (VUR) was detected. The authorship required at least one pediatrician or surgeon. Authorship was categorized as medical, surgical, or combined.
Pediatricians advocated less imaging and intervention and were more inclined to adopt a "watchful-waiting" approach, confident that any significant abnormality, grades IV-V VUR in particular, should be detected following a second febrile UTI. In contrast, surgeons were more likely to recommend imaging to detect VUR (p<0.00001), and antibiotic prophylaxis (p<0.001) and/or surgical correction (p=0.004) if it was detected, concerned that any delay in diagnosis and treatment could place the child at risk of kidney damage. Papers with combined authorship displayed intermediate results.
There are two distinct directions in the literature regarding the investigation of an uncomplicated first febrile UTI in a child. In general, when presented with a first febrile UTI in a child, physicians recommend fewer investigations and less treatment, in contrast to surgeons who advocate extensive investigation and aggressive intervention in the event that imaging detects an abnormality. This has the potential to confuse the carers of affected children.
儿童首次发热性尿路感染(UTI)是一种常见病症,其管理途径随着时间的推移而演变。
确定儿科医生和外科医生在首次发热性 UTI 的检查和管理方面的差异程度,并评估任何方法差异的理由。
对 2011 年至 2021 年期间发表的关于儿童首次发热性 UTI 后检查和/或管理的论文进行了文献检索。在 Medline、Embase 和 Cochrane 对照试验登记处进行了检索。为了符合纳入标准,一篇论文必须就以下一项或多项提供建议:超声(US)和排尿性膀胱尿道造影(VCUG)、当检测到膀胱输尿管反流(VUR)时需要持续使用抗生素预防和手术。作者至少有一名儿科医生或外科医生。作者分类为医学、外科或综合。
儿科医生主张减少影像学检查和干预,更倾向于采用“观察等待”的方法,他们相信任何显著异常,特别是 IV-V 级 VUR,都应该在第二次发热性 UTI 后被发现。相比之下,外科医生更有可能建议进行影像学检查以检测 VUR(p<0.00001),并建议使用抗生素预防(p<0.001)和/或手术矫正(p=0.004)如果检测到 VUR,他们担心任何诊断和治疗的延迟都可能使孩子面临肾脏损伤的风险。具有综合作者的论文显示出中间结果。
在儿童简单的首次发热性 UTI 的检查方面,文献中有两种截然不同的方向。一般来说,当儿科医生面对儿童的首次发热性 UTI 时,他们建议进行较少的检查和治疗,与主张在影像学检查发现异常时进行广泛检查和积极干预的外科医生形成对比。这可能会使受影响儿童的照顾者感到困惑。