Sun Yongkang, Lian Feng, Deng Yuanyuan, Liao Sha, Wang Ying
Department of Ultrasound, Seventh People's Hospital of Shanghai University of Traditional Chinese Medicine, Shanghai, 200137, PR China.
Heliyon. 2023 Sep 27;9(10):e20453. doi: 10.1016/j.heliyon.2023.e20453. eCollection 2023 Oct.
Spontaneous preterm birth (sPTB) stands as a leading cause of neonatal mortality. Consequently, preventing sPTB has emerged as a paramount concern in healthcare. Therefore, our study aimed to develop a nomogram, encompassing patient characteristics and cervical elastography, to predict sPTB in singleton pregnancies. Specifically, we targeted those with a short cervix length (CL), no history of sPTB, and who were receiving vaginal progesterone therapy.
A total of 568 patients were included in this study. Data from 392 patients, collected between January 2016 and October 2019, constituted the training cohort. Meanwhile, records from 176 patients, spanning November 2019 to January 2022, formed the validation cohort. Following the univariate logistic regression analysis, variables exhibiting a P-value less than 0.05 were integrated into a multivariable logistic regression analysis. The primary objective of this subsequent analysis was to identify the independent predictors linked to sPTB in the training cohort. Next, we formulated a nomogram utilizing the identified independent predictors. This tool was designed to estimate the likelihood of sPTB in singleton pregnancies, particularly those with a short CL, devoid of any sPTB history, and undergoing vaginal progesterone therapy. The C-index, Hosmer-Lemeshow (HL) test, calibration curves, decision curve analysis (DCA), and receiver operating characteristic (ROC) were used to validate the performance of the nomogram.
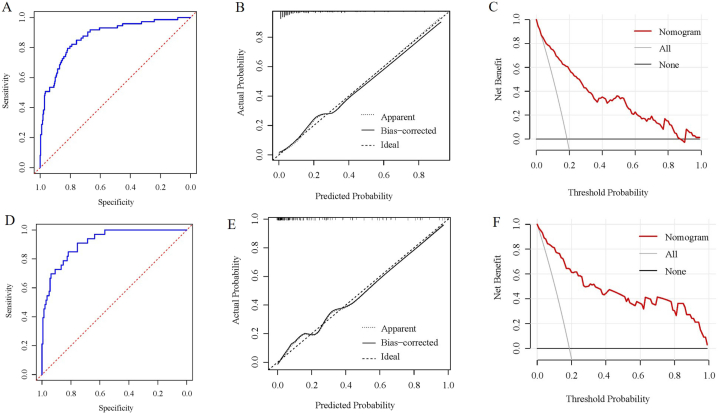
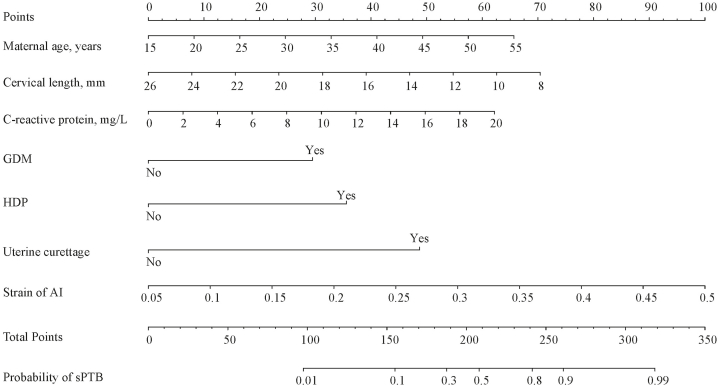
Upon finalizing the univariate analysis, we progressed to a multivariable analysis, integrating 8 variables with P < 0.05 from the univariate analysis. The multivariable analysis identified 7 independent risk factors: maternal age (OR = 1.072; P < 0.001), cervical length (OR = 0.854; P < 0.001), uterine curettage (OR = 7.208; P < 0.001), GDM (OR = 3.570; P = 0.006), HDP (OR = 4.661; P = 0.003), C-reactive protein (OR = 1.138; P < 0.001), and strain of AI (OR = 7.985; P < 0.001). The nomogram, tailored for sPTB prediction, was grounded on these 7 independent predictors. In predicting sPTB, the C-indices manifested as 0.873 (95% CI, 0.827-0.918) for the training cohort and 0.916 (95%CI, 0.870-0.962) for the validation cohorts, underscoring a good discrimination of the model. Additionally, the ROC curves served to evaluate the discrimination of nomogram model across both cohorts. Calibration curves were delineated, revealing no statistically significant differences in both the training (χ = 5.355; = 0.719) and validation (χ = 2.708; = 0.951) cohorts as evidenced by the HL tests. Furthermore, the DCA underscored the model's excellence as a predictive tool for sPTB.
By amalgamating patient characteristics and cervical elastography data from the second trimester, the nomogram emerged as a visually intuitive and dependable tool for predicting sPTB. Its relevance was particularly pronounced for singleton pregnancies characterized by a short CL, an absence of prior sPTB incidents, and those receiving vaginal progesterone therapy.

自发性早产(sPTB)是新生儿死亡的主要原因。因此,预防sPTB已成为医疗保健领域的首要关注点。因此,我们的研究旨在开发一种列线图,纳入患者特征和宫颈弹性成像,以预测单胎妊娠中的sPTB。具体而言,我们针对宫颈长度(CL)短、无sPTB病史且正在接受阴道孕酮治疗的患者。
本研究共纳入568例患者。2016年1月至2019年10月收集的392例患者的数据构成训练队列。同时,2019年11月至2022年1月期间176例患者的记录形成验证队列。在单因素逻辑回归分析之后,将P值小于0.05的变量纳入多因素逻辑回归分析。后续分析的主要目的是确定训练队列中与sPTB相关的独立预测因素。接下来,我们利用确定的独立预测因素制定了一个列线图。该工具旨在估计单胎妊娠中sPTB的可能性,特别是那些CL短、无任何sPTB病史且正在接受阴道孕酮治疗的妊娠。使用C指数、Hosmer-Lemeshow(HL)检验、校准曲线、决策曲线分析(DCA)和受试者操作特征(ROC)来验证列线图的性能。
在完成单因素分析后,我们进行了多因素分析,纳入了单因素分析中P<0.05的8个变量。多因素分析确定了7个独立危险因素:产妇年龄(OR = 1.072;P < 0.001)、宫颈长度(OR = 0.854;P < 0.001)、刮宫术(OR = 7.208;P < 0.001)、妊娠期糖尿病(GDM,OR = 3.570;P = 0.006)、妊娠期高血压疾病(HDP,OR = 4.661;P = 0.003)、C反应蛋白(OR = 1.138;P < 0.001)和AI应变(OR = 7.985;P < 0.001)。针对sPTB预测量身定制的列线图基于这7个独立预测因素。在预测sPTB时,训练队列的C指数为0.873(95%CI,0.827 - 0.918),验证队列的C指数为0.916(95%CI,0.870 - 0.962),表明该模型具有良好的区分度。此外,ROC曲线用于评估列线图模型在两个队列中的区分度。绘制了校准曲线,HL检验表明训练队列(χ = 5.355;P = 0.719)和验证队列(χ = 2.708;P = 0.951)均无统计学显著差异。此外,DCA强调了该模型作为sPTB预测工具的卓越性。
通过整合孕中期的患者特征和宫颈弹性成像数据,列线图成为预测sPTB的直观且可靠的工具。其相关性在CL短、既往无sPTB事件且接受阴道孕酮治疗的单胎妊娠中尤为明显。